")
")
")
")
")
to view the full video presentation register for the certification course” www.scoliosisandspineonlinelearning.com
 |
|
 |
Scoliosis does not only affect the spine, it will also lead to a deformation of the rib cage. Minor deformities must be taken into account when making braces. |
 |
. |
 |
The rib hump is a deformity characteristic of scoliosis, usually right thoracic, it is accompanied by a left anterior thoracic contra-rib hump and it is often the deformity that the child will notice. |
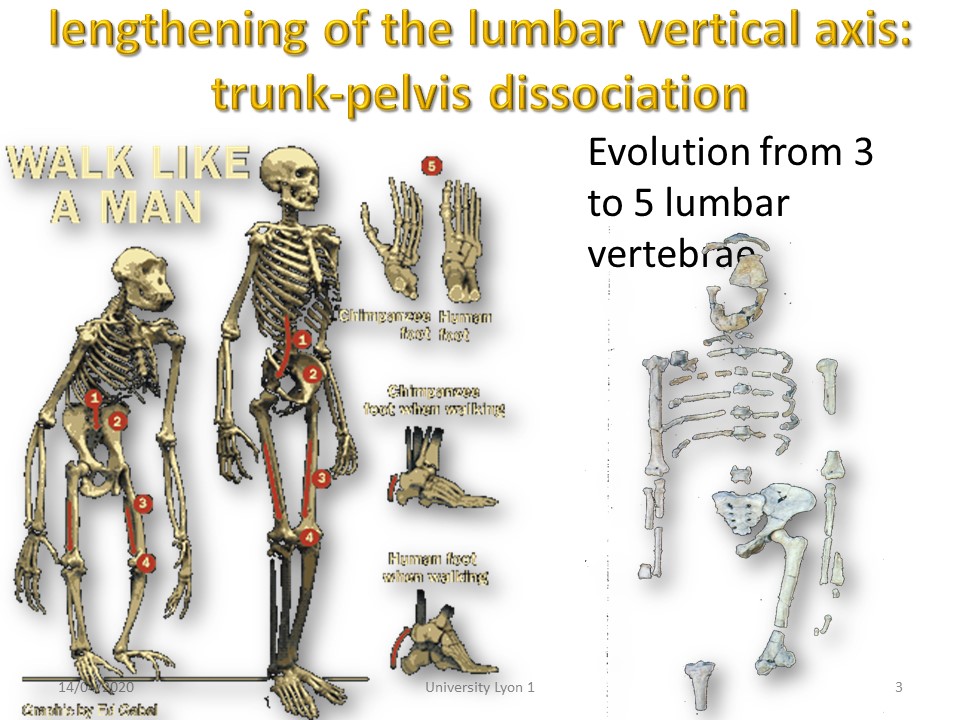 |
With Homo sapiens, the rib cage gradually dissociates from the pelvis, passing from 3 to 5 lumbar vertebrae. The volume also changes from a funnel shape to a cone shape. |
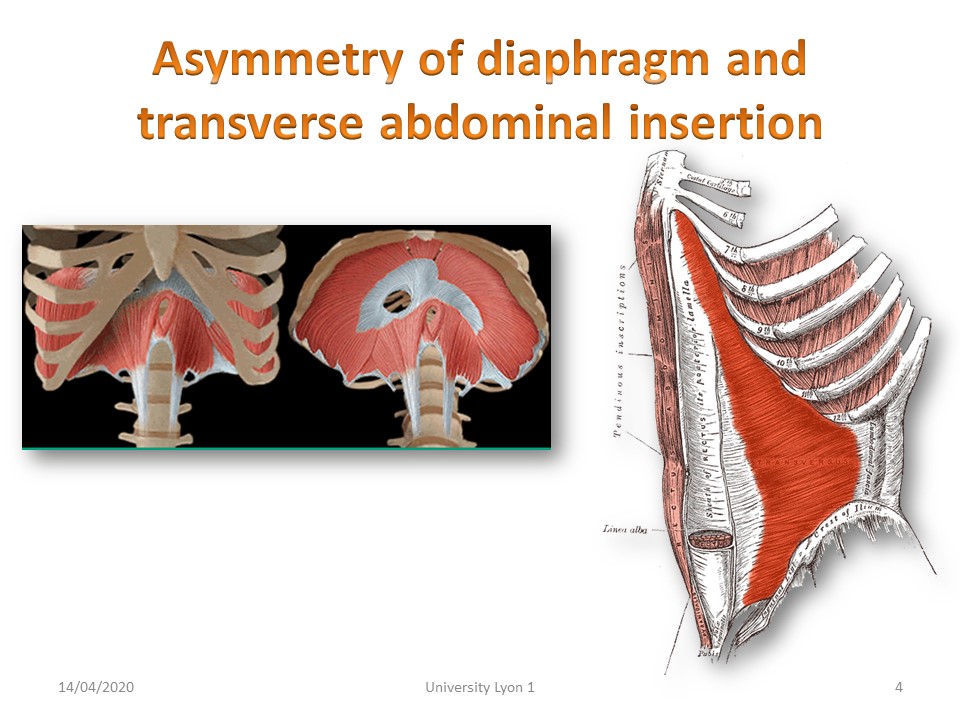 |
The lower sternal deformities appear to be related to an insertion asymmetry of the diaphragm and transversus abdominalis. |
 |
. |
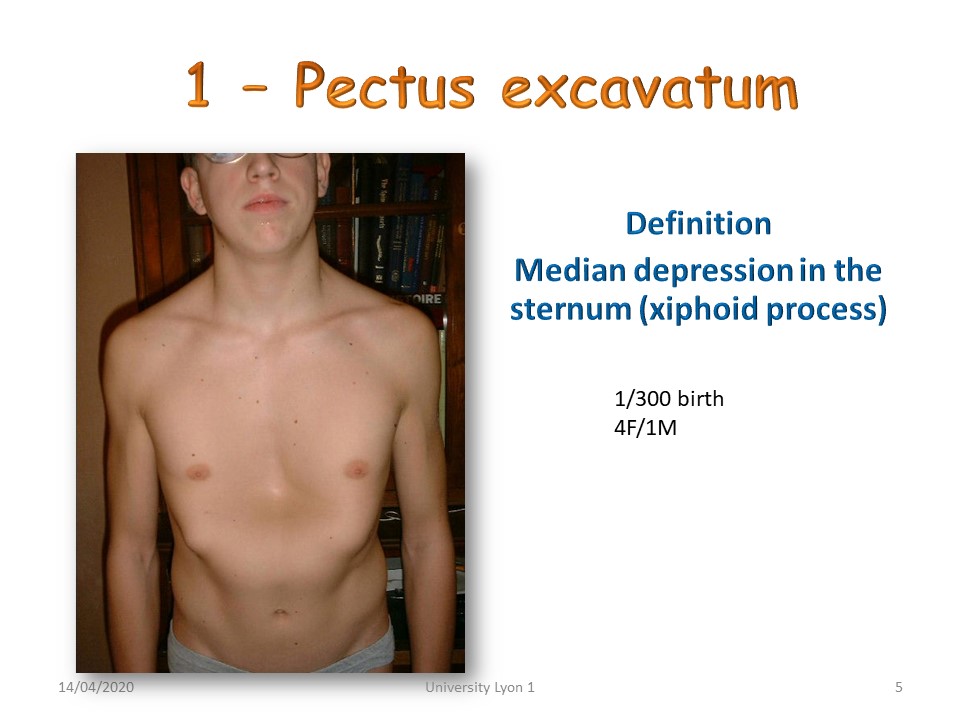 |
One of the most frequent (1/300) is the pectus excavatum with median depression of the sternum at the level of the xyphoid appendix. It concerns 4 girls for 1 boy. |
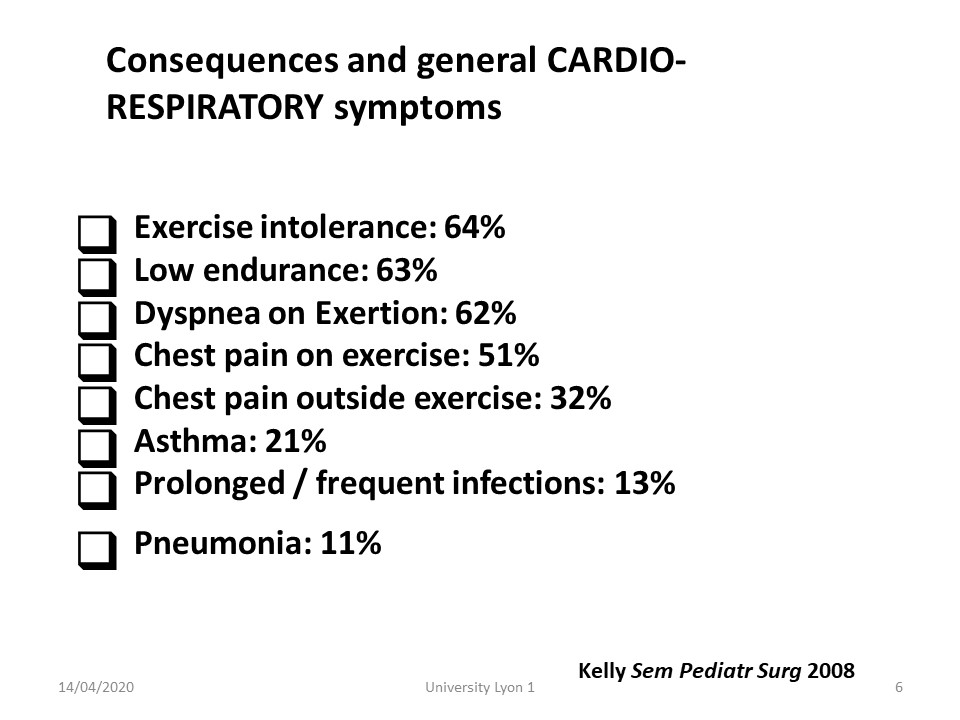 |
The most important deformities lead to cardio-pulmonary symptomatology with breathing difficulties on effort and pulmonary infections. It is in these forms that surgical indications will be discussed, |
 |
In some cases, a fetal origin has been evoked with imprints of the baby's fists on the sternum at the end of pregnancy. |
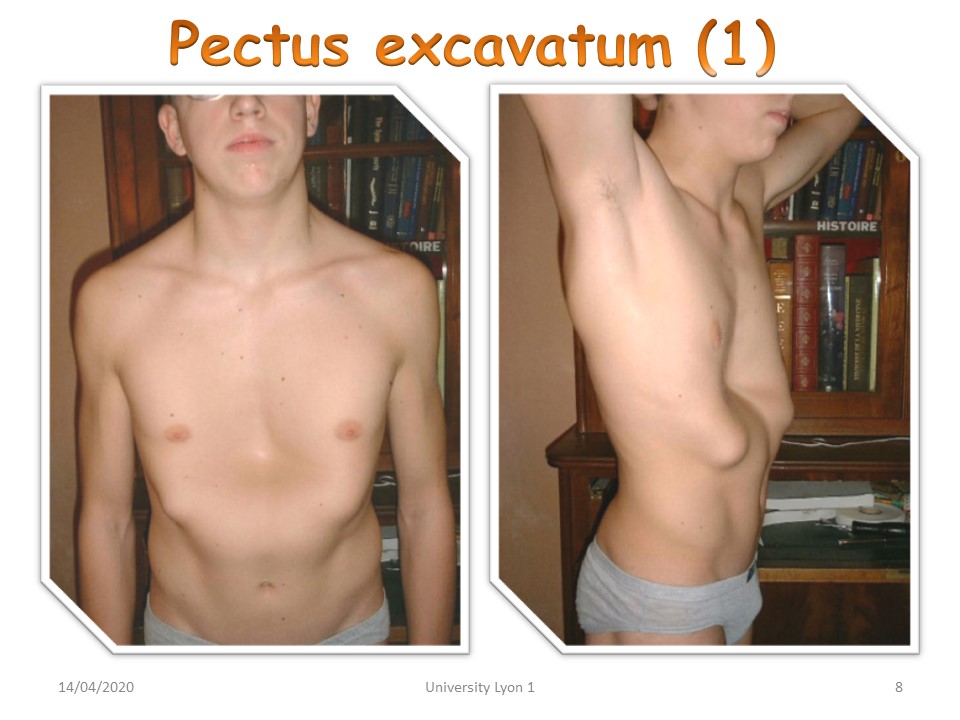 |
This median sternal depression is often associated with a protrusion of the chondro-costal awnings at a vertical line passing through the nipples. These are the "Sigaud's ailerons", |
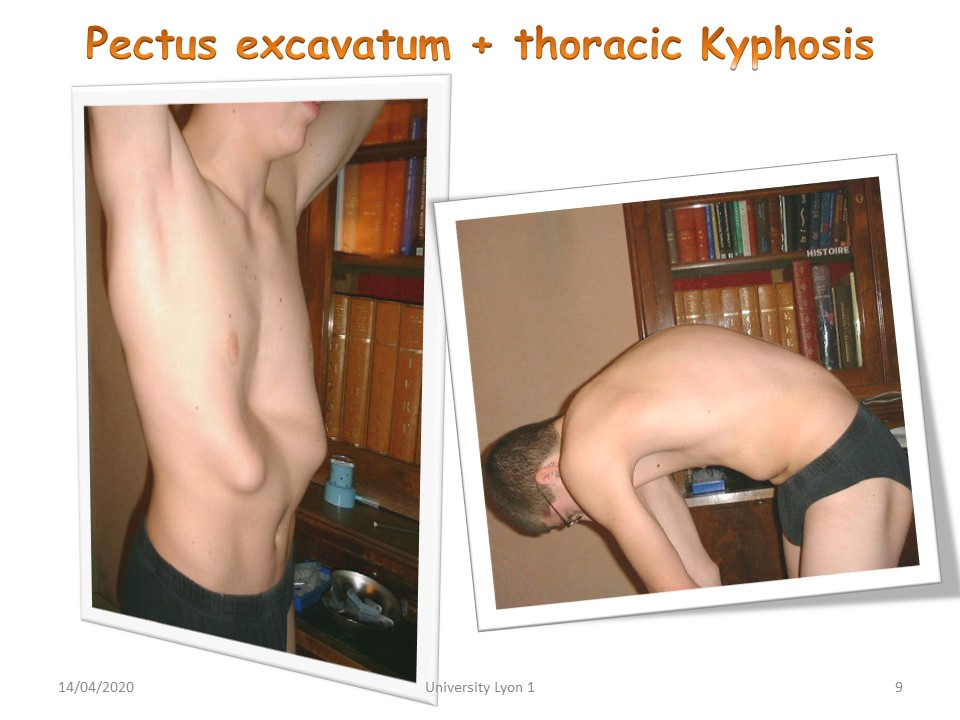 |
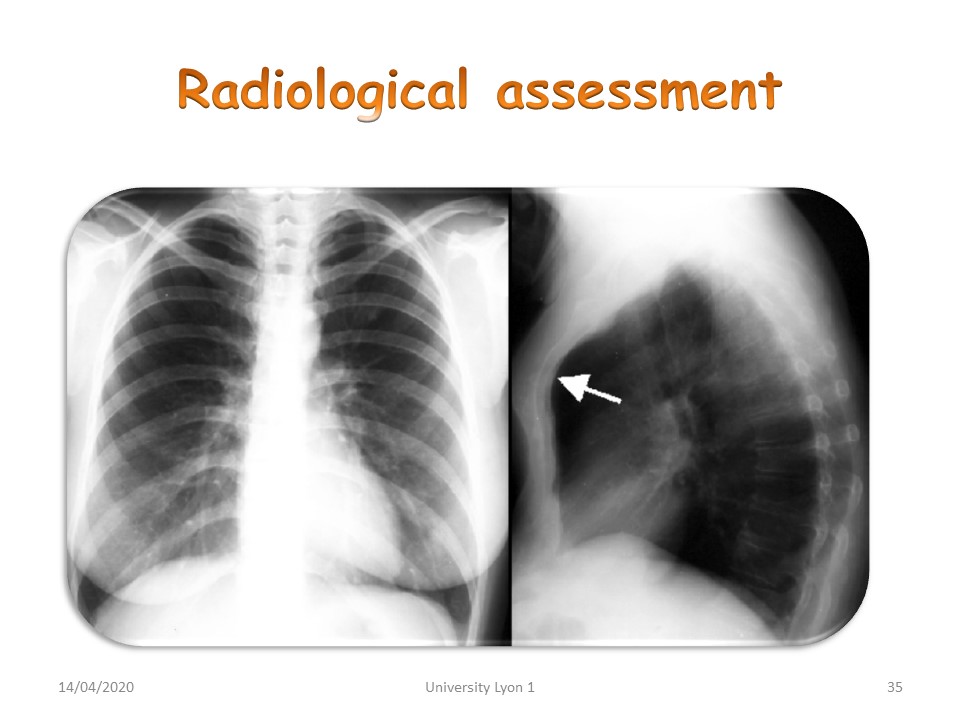
Anterior depression may be associated with posterior kyphosis, which increases the distance between the sternum and the anterior wall of the vertebral body. Care must therefore be taken to avoid reducing this distance by an overly corrective brace. |
 |
Profile X-rays measure this distance between the sternum and the anterior wall of the vertebral body, usually at the thoracolumbar junction. If the apex of the kyphosis is higher in T7, it is possible to make a brace with high sterno-clavicular support and simple contact without correction at the basis of the rib cage. |
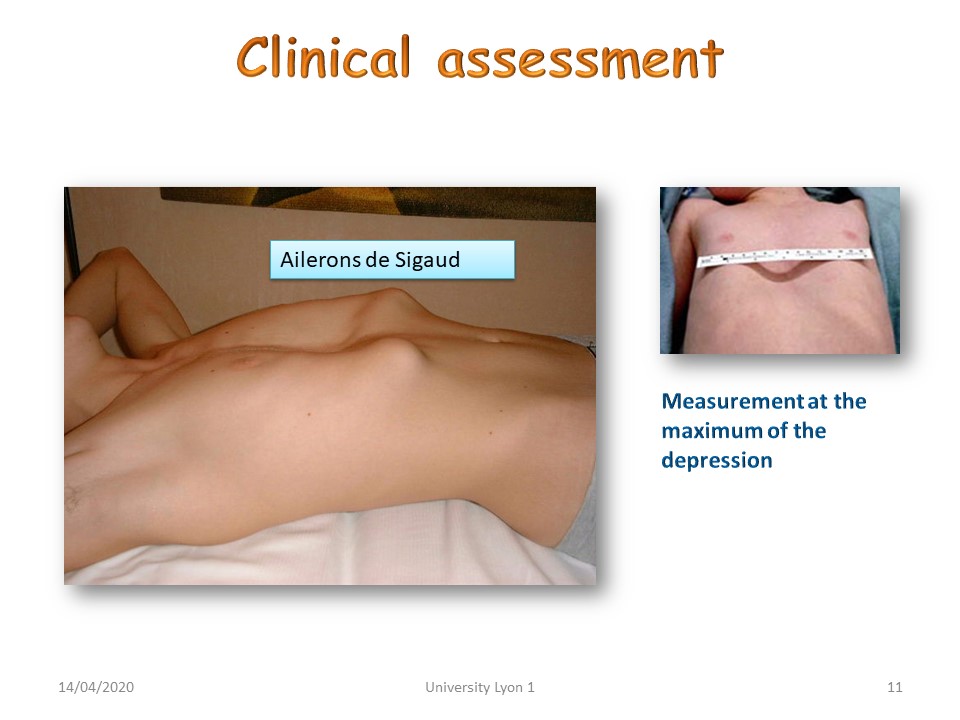 |
The depression is measured at the maximum of the depression from the chondro-costal awnings, i.e. taking both deformations into account. |
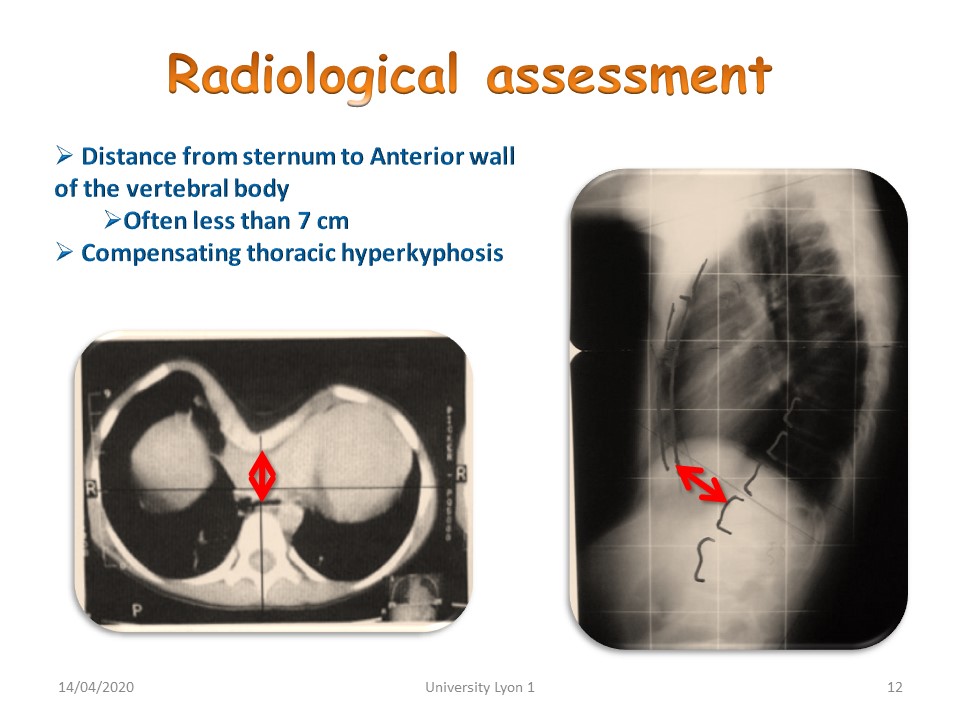 |
The scanner with horizontal slices at the maximum depression allows a more precise measurement and also shows asymmetries in the frontal plane. |
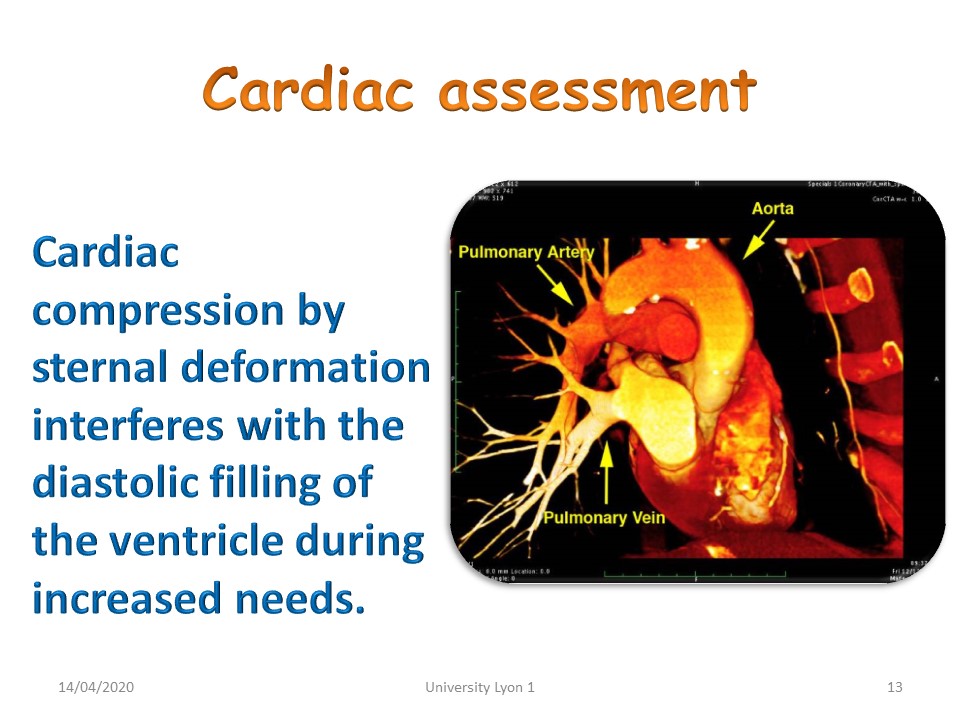 |
The cardiac check-up may reveal an abnormal diastolic filling of the ventricle during exercise. |
 |
But most of the time the electrocardiographic signs are atypical, such as hypertrophy or repolarization disorders. |
 |
Pulmonary signs are also atypical such as exercise dyspnea, lung infections or asthma. |
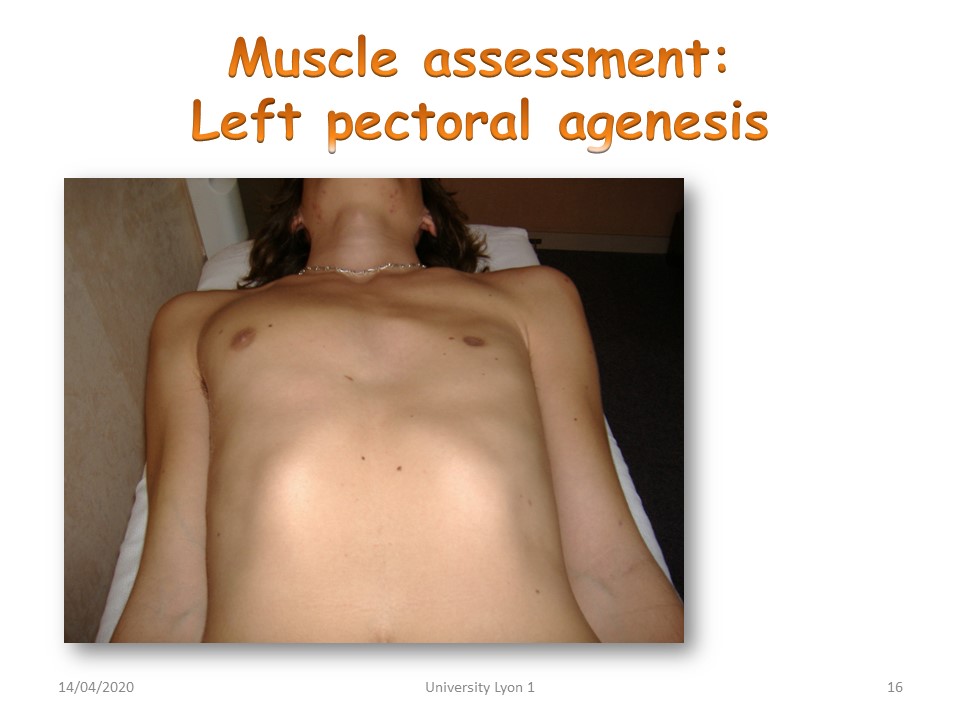 |
The asymmetry is not always bony, it can also be muscular with pectoralis agenesis. We'll look for other deformities in the context of Poland Syndrome. |
 |
The physiotherapy assessment will look for a median depression in the infant that becomes more pronounced when the child cries and sometimes protrusion and elevation of the lower ribs. The abdominal muscles may be hypotonic. In an older child, decreased chest expansion and stiffness may be seen. |
 |
Physiotherapy will focus on strengthening the abdominal muscles from the decubitus to the sitting position in very small children. Regarding depression bells, long-term results are not published. |
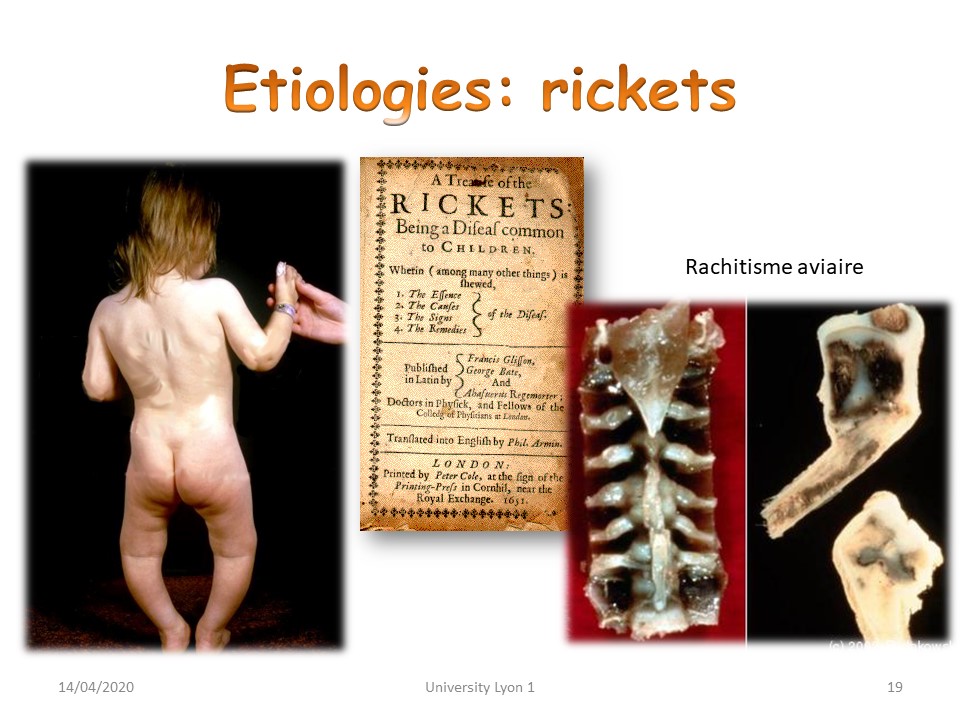 |
Thoracic deformities were common in the era of rickets. |
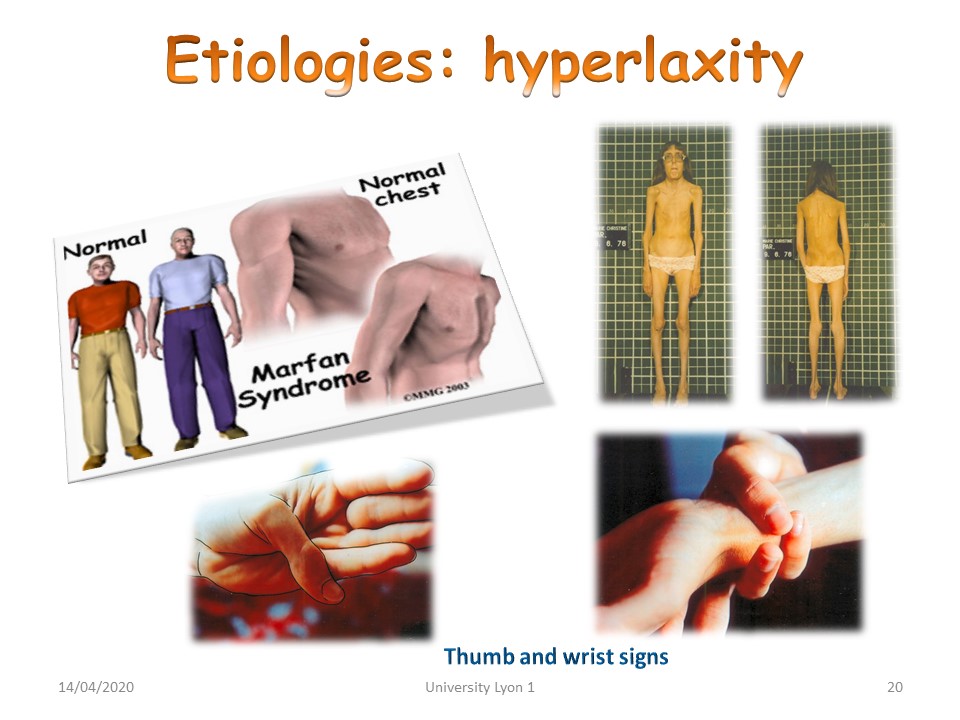 |
Currently, thoracic deformities are frequently associated with genetic syndromes such as Marfan's disease. |
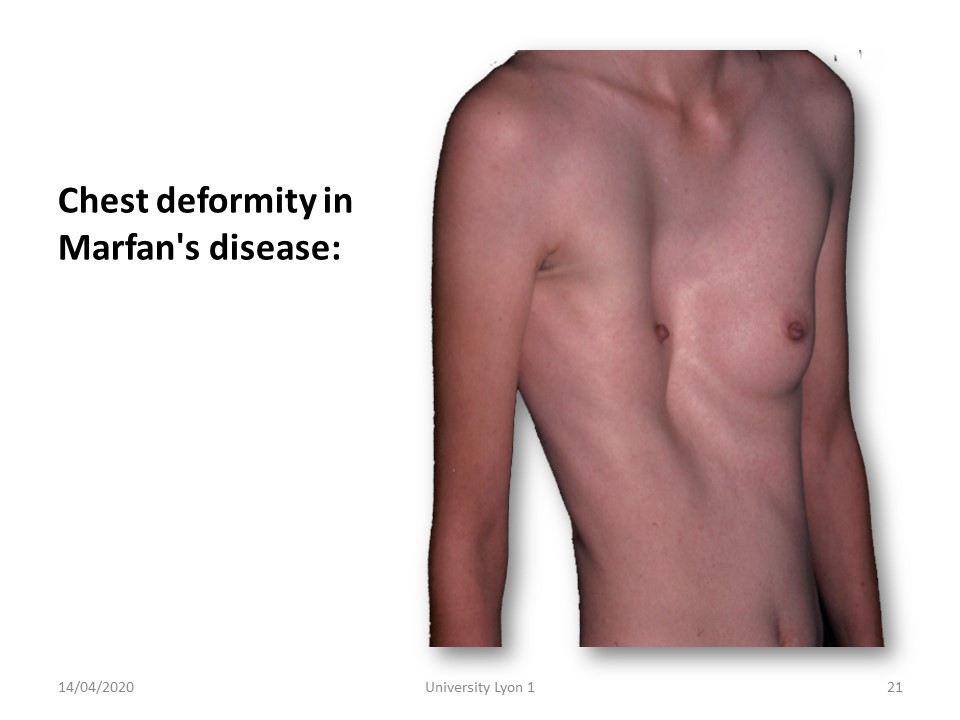 |
The deformations may be asymmetrical. |
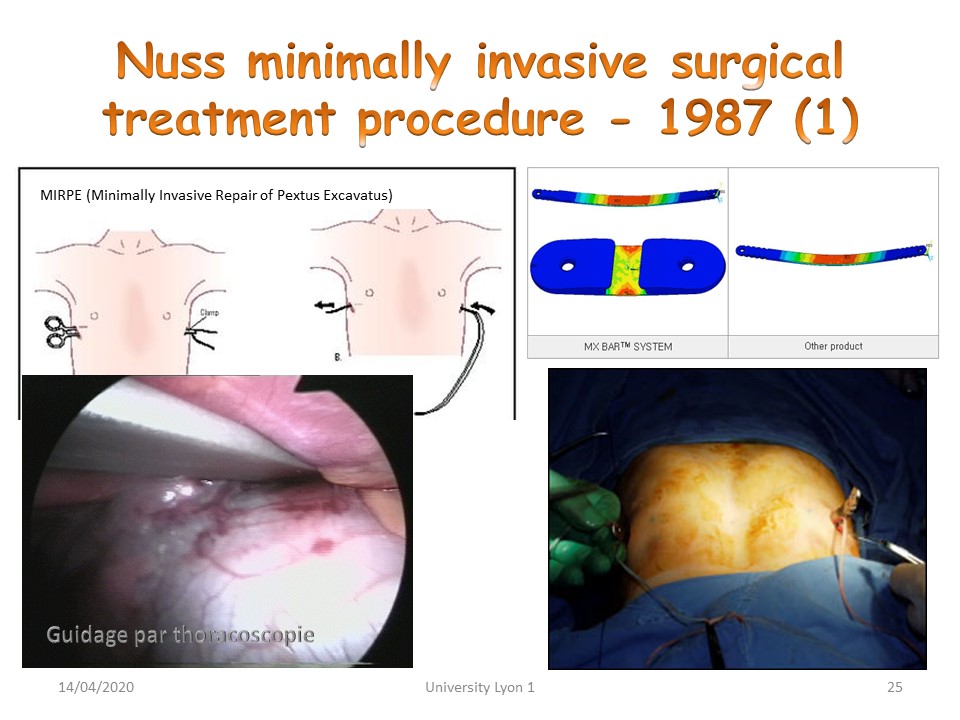 |
In the most important cases of pectus excavatum with functional limitation, there is little alternative to surgery. The least invasive technique is the one described by Nuss which is performed under thoracoscopy. |
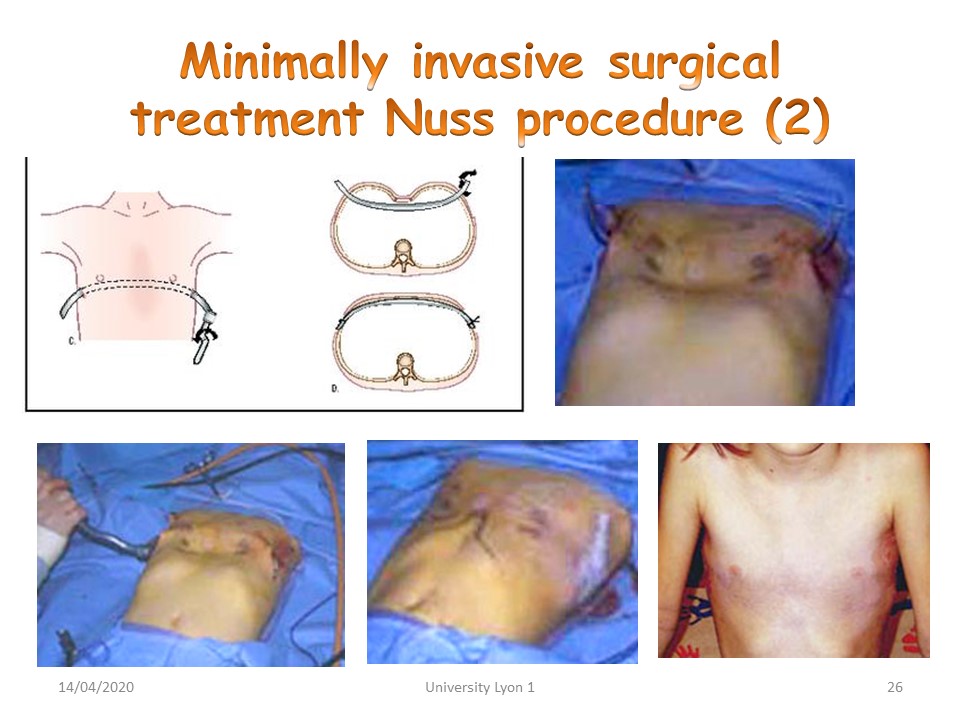 |
The metal bar is preformed according to the CT scan performed before surgery and will be turned 180° during the procedure. |
 |
The bar is kept for at least 6 months and care must be taken to ensure analgesic treatment after surgery. |
 |
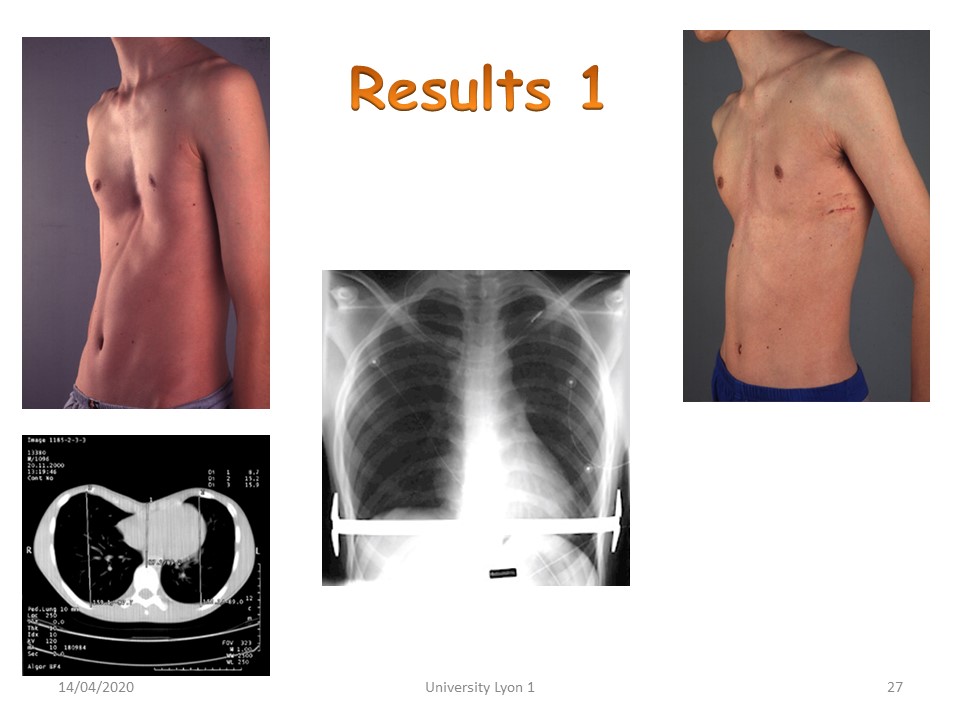
Physiotherapy will be carried out during the first 6 weeks after surgery. Breathing exercises are aimed at avoiding scar adhesions and pulmonary infections. |
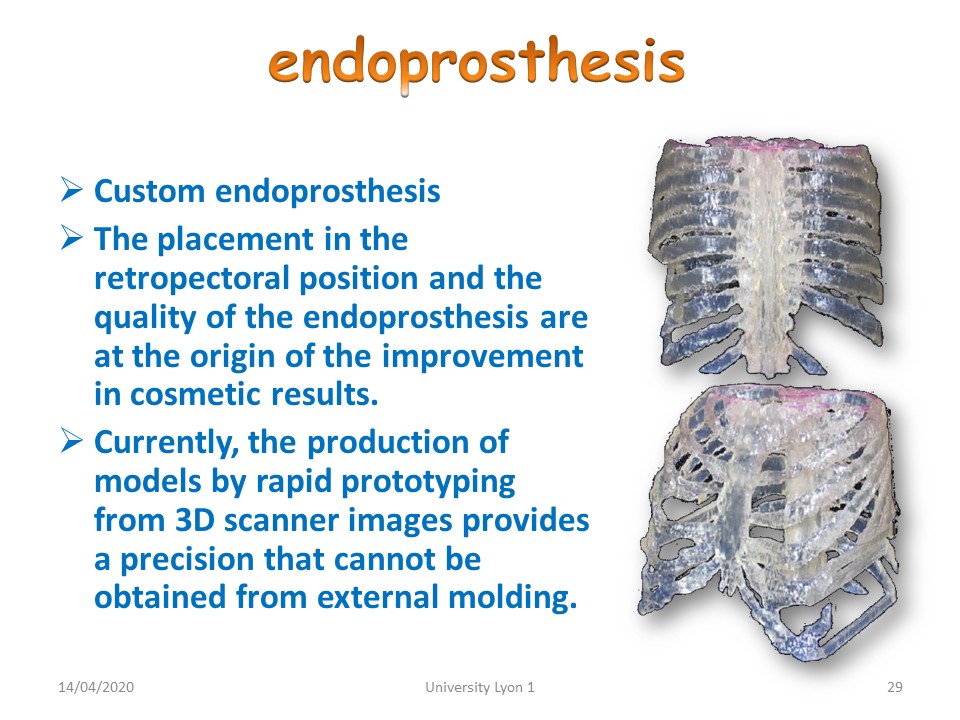 |
Where there is no functional limitation, the problem is essentially aesthetic. In girls, the development of the breast’s masks most of the deformities, in boys, it is then possible to make endoprosthesis that will be placed under the skin. |
 |
|
 |
Recklinghausen's disease is a phacomatosis and affects tissues derived from the ectoderm. The presence of more than 7 café au lait spots is characteristic, Thoracic deformities associated with scoliosis are often greater than in idiopathic scoliosis. |
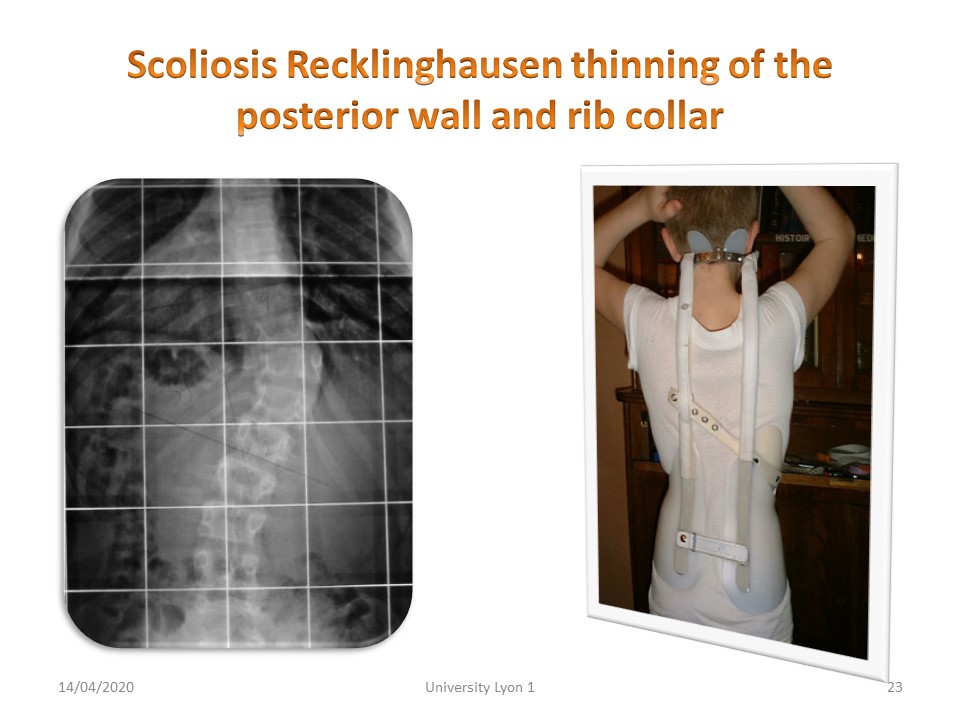 |
Scoliosis involves a thinning of the posterior wall of the vertebral body and the neck of the ribs, the embryology of which is derived from the ectoderm. This narrowing widens the medullary canal and avoids neurological complications. The posterior arch remains intact, which limits extension. The curvatures are short and make fitting difficult. |
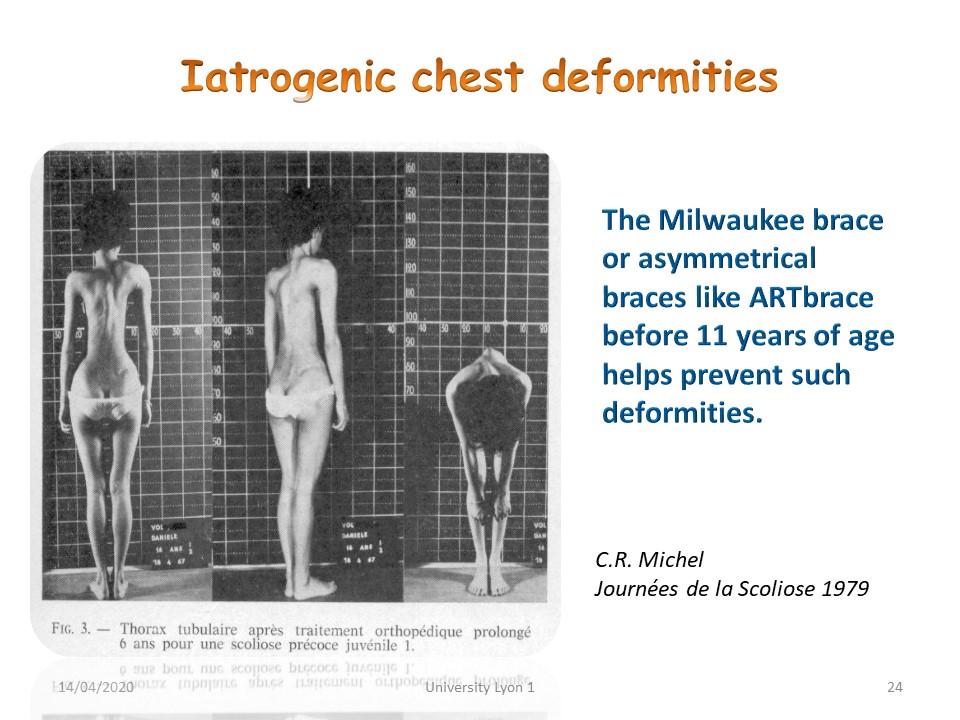 |
Iatrogenic thoracic deformities favoured by the wearing of a brace during the pulmonary development phase, the first three years of life, should also be mentioned. |
 |
. |
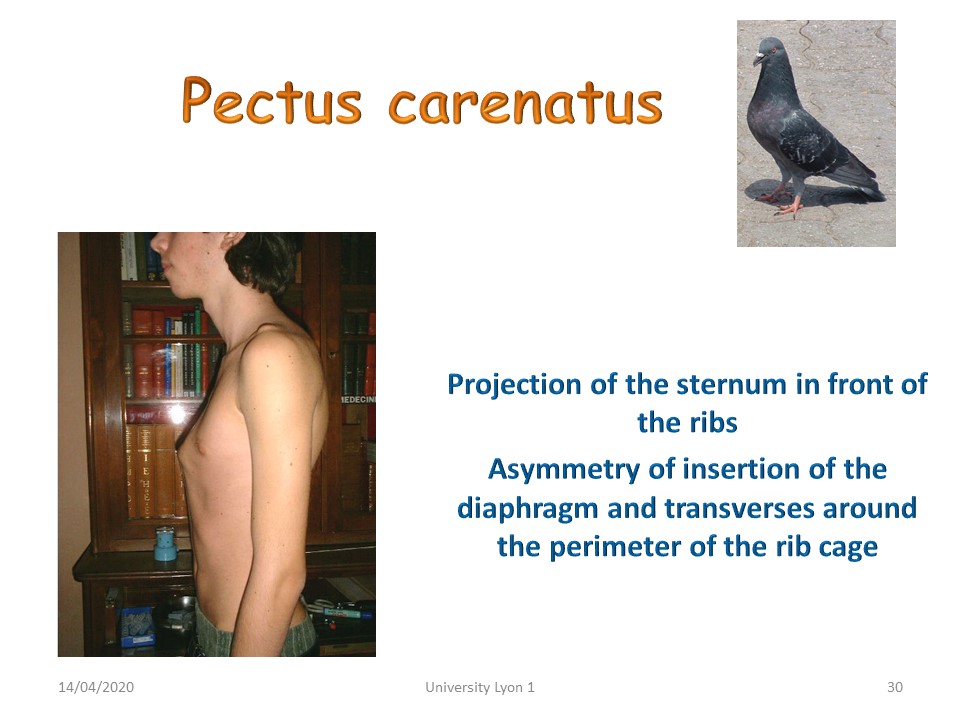 |
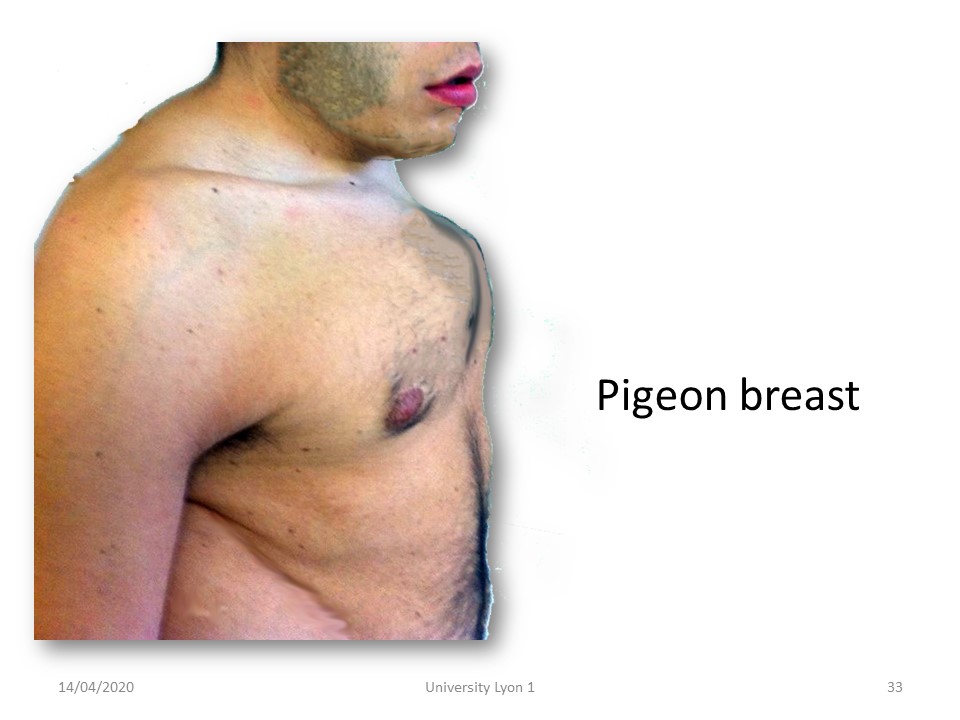
Conversely, the forward projection of the sternum is much easier to shape with a brace. |
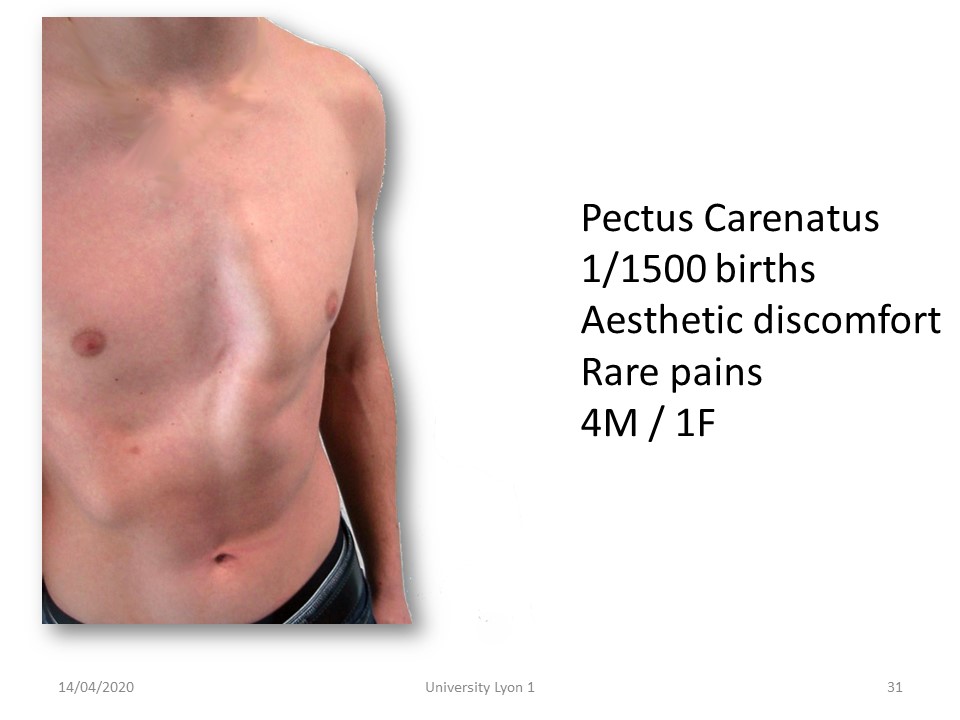 |
The pectus carinatum can be asymmetrical, which accentuates the cosmetic appearance. |
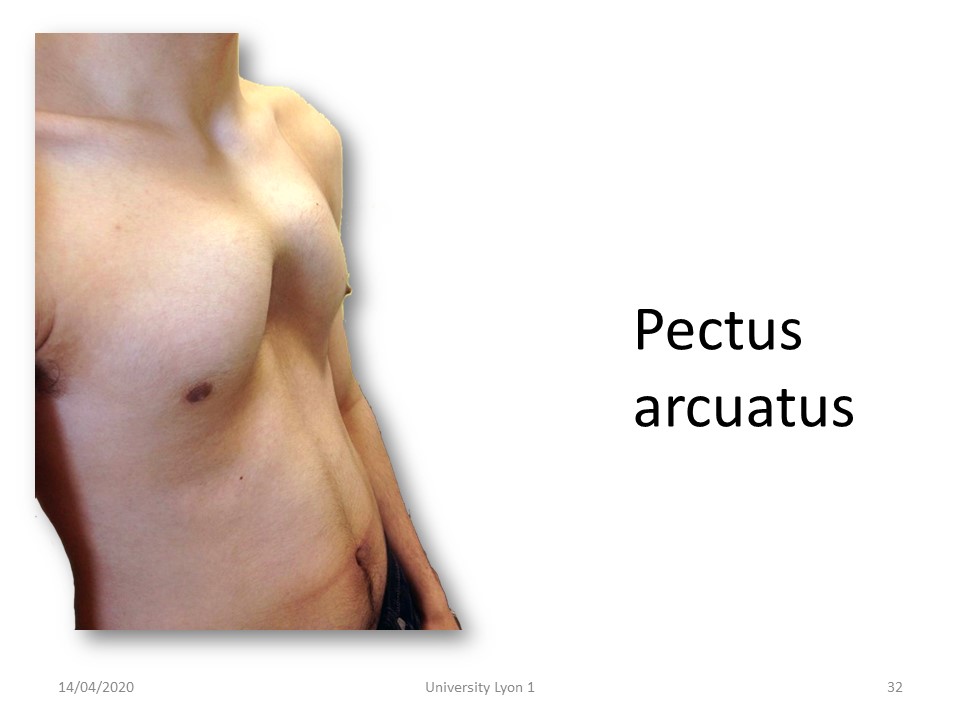 |
The deformities can be located in different parts of the thorax with an arched shape. |
 |
The deformity sometimes forms a 90° angulation at the sternum. |
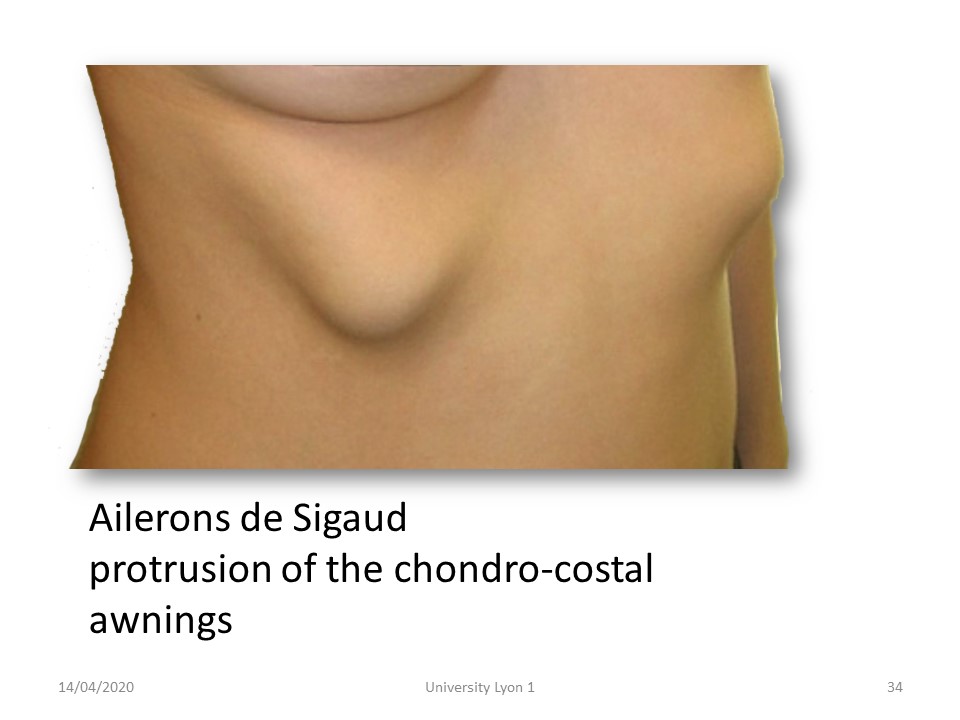 |
The protrusion of chondro-costal awnings can easily be shaped by a night brace. |
 |
The contour of the bone deformity is usually clearly visible radiologically. |
 |
Small night-time 3-point systems are effective but require a good adaptation to avoid moving at night. |
 |
In general, there is no functional limitation in the pectus carinatum, so plastic surgery will be reserved for a few exceptional cases. |
Comment in the certification part of the website
|
|
 |
|
 |
Only thoracic curvatures have the potential to alter lung function. But small thoracic curvatures between 20 and 45 degrees may decrease lung function during intense exercise. |
 |
In scoliosis, this is not a weakness of the diaphragm muscle, but more a limitation of costovertebral mobility and torsional asymmetry of the rib-cage base, |
 |
Usually there is a decrease in expiratory reserve volume, decreased movement during breathing and asymmetry of diaphragm movement. |
 |
Pulmonary function is impaired in very severe scoliosis with an increase in trans-diaphragmatic pressures and a limitation of pressures in maximum inspiration or expiration. |
 |
For Schroth, an AIS patient suffers from an uneven distribution of ventilations defining hypo and hyperventilated thoracic zones (concavity and convexity) and that the exercises of her method generate a corrective vertebral derotation by voluntary and directed increase of the ventilation in the areas of concavity. |
 |
However, Mahaudens demonstrates there was no unequal distribution of splitting between flats and rib hump in AIS subjects. The Schroth method directs the ventilation towards the flats, but without modifying the homogeneous ratio of the splits between flats and rib hump. |
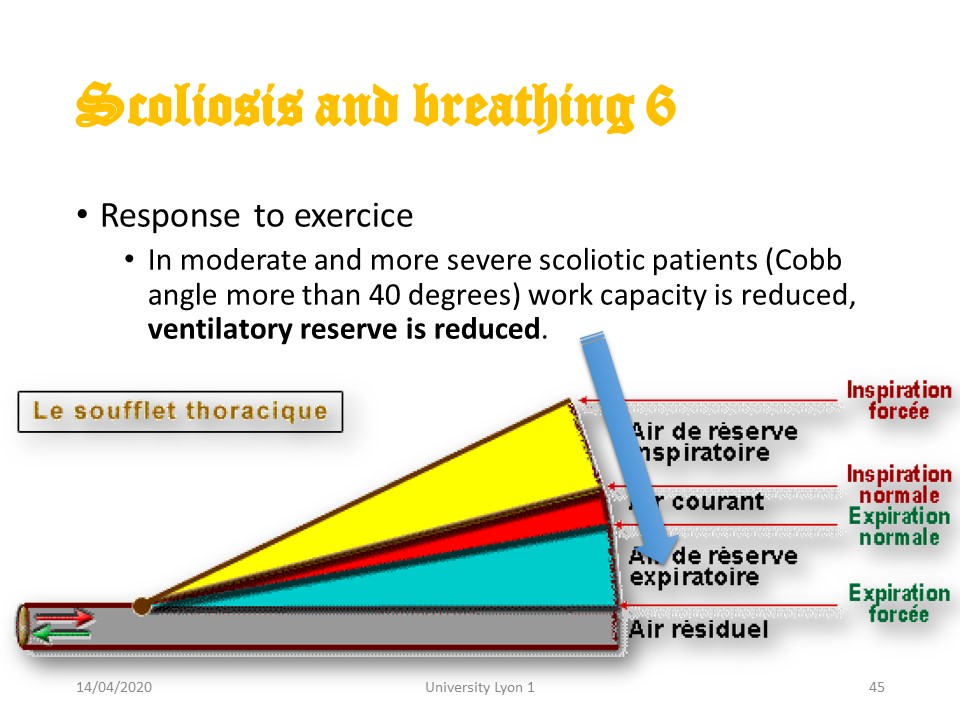 |
In the Lyon method, respiratory physiotherapy has always been carried out in the sense of increasing the expiratory reserve volume. |
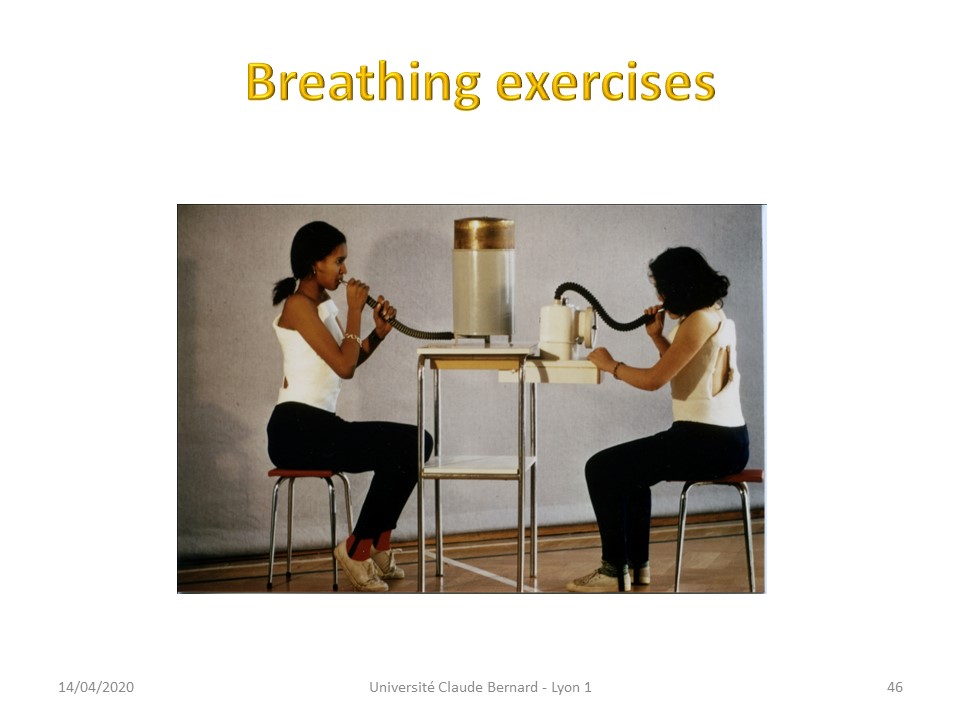 |
The child is asked to blow as much air as possible into the spirometer. The advantage is that he can control his progress. |
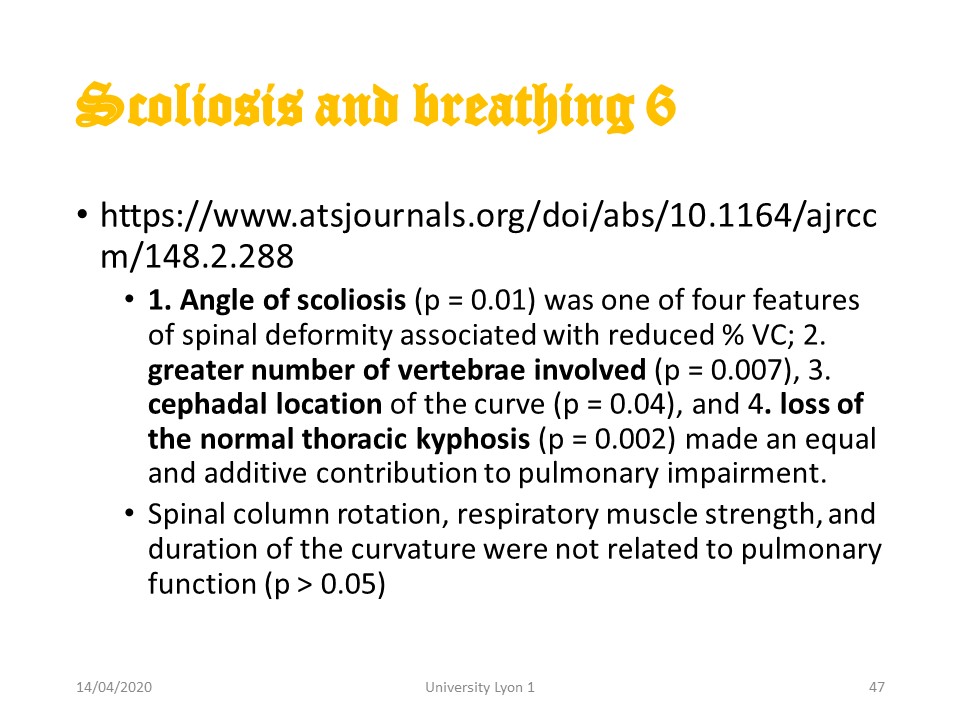 |
Factors that contribute to respiratory discomfort are the angulation of the curvature, the number of vertebrae involved, the high location of the scoliosis and the flat back. |
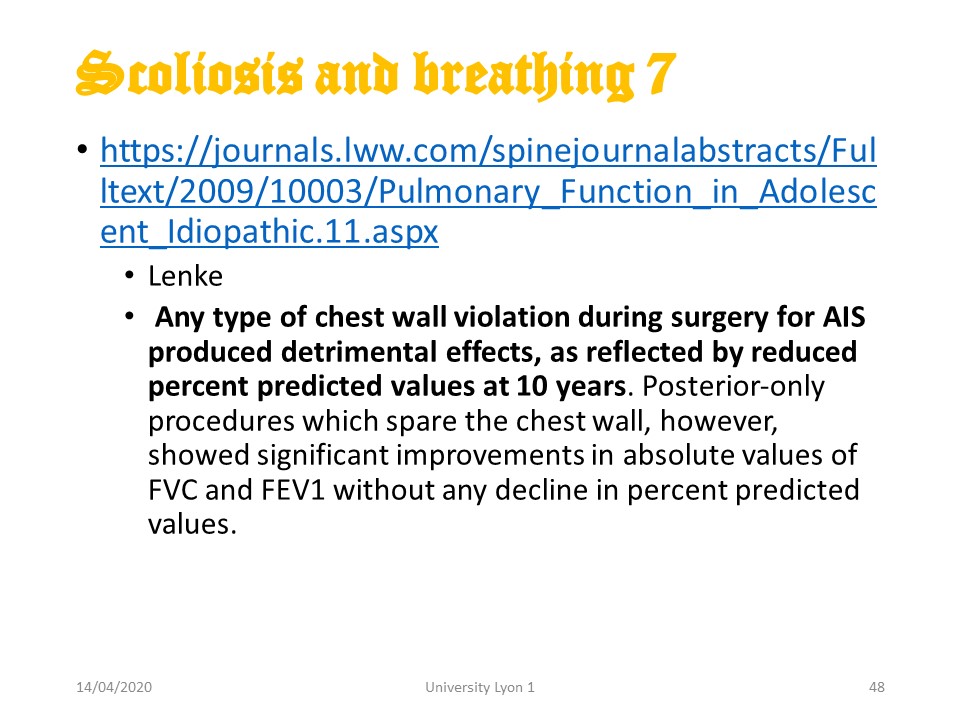 |
Thoracotomies have a greater impact on vital capacity, but even posterior arthrodesis surgery reduces vital capacity by about 20% and may require specific physiotherapy. |
 |
|
Comment in the certification part of the website
|
|
 |
The impact of ARTbrace on vital capacity was measured. The spirometry tests were performed using SP10 Contec. |
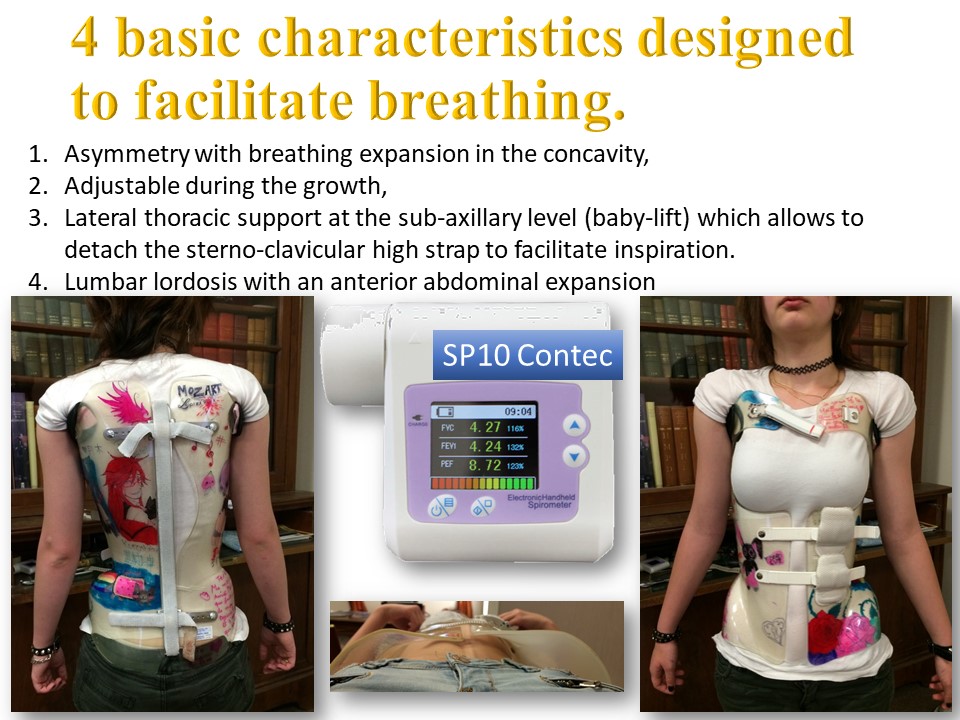 |
4 basic characteristics designed to facilitate breathing. 1. Asymmetry with breathing expansion in the concavity. 2. The brace is adjustable during the growth. 3. Lateral thoracic contact at the under-arm level (baby-lift) which allows to detach the sterno-clavicular high strap to facilitate inspiration. 4. Lumbar lordosis with an anterior abdominal expansion. |
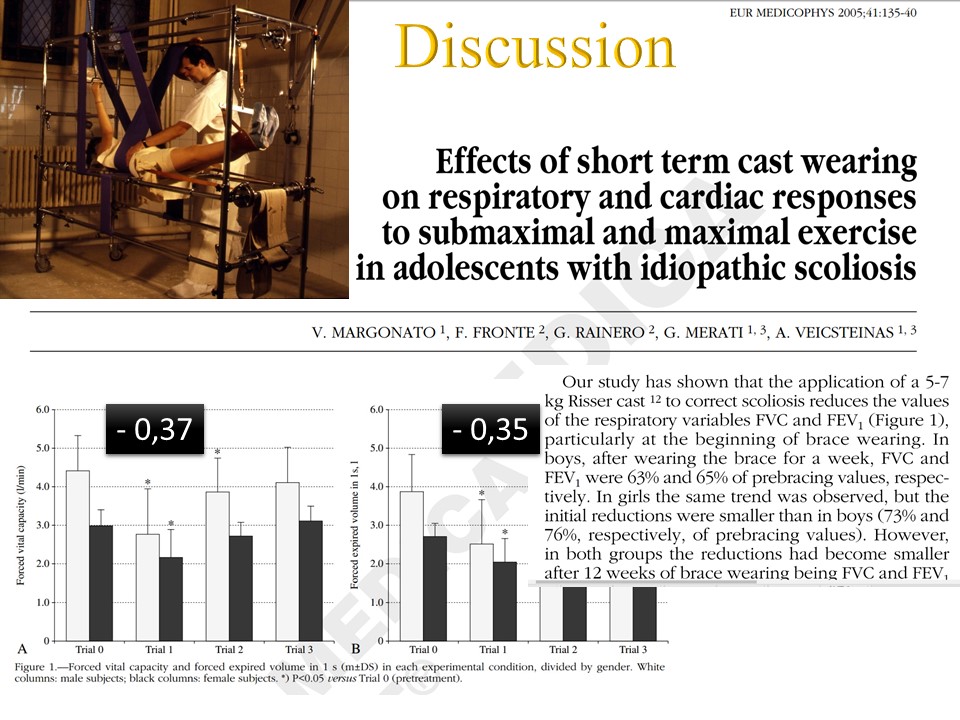 |
The restriction of the vital capacity was more than 35% in plaster cast. |
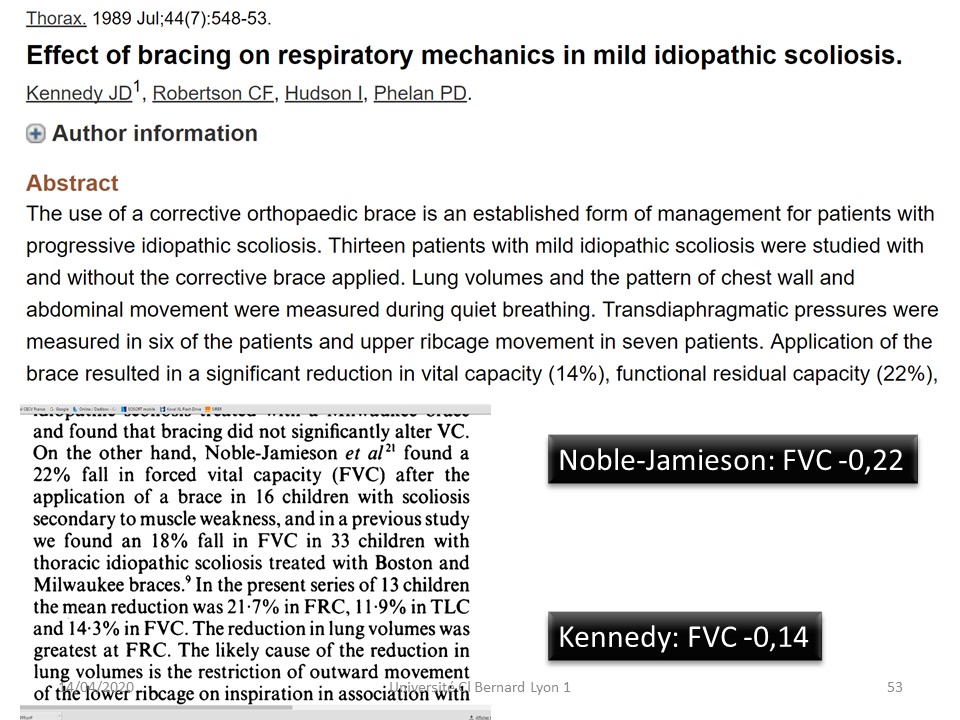 |
In braces, the limitation varies from 22 to 14% according to international publications. |
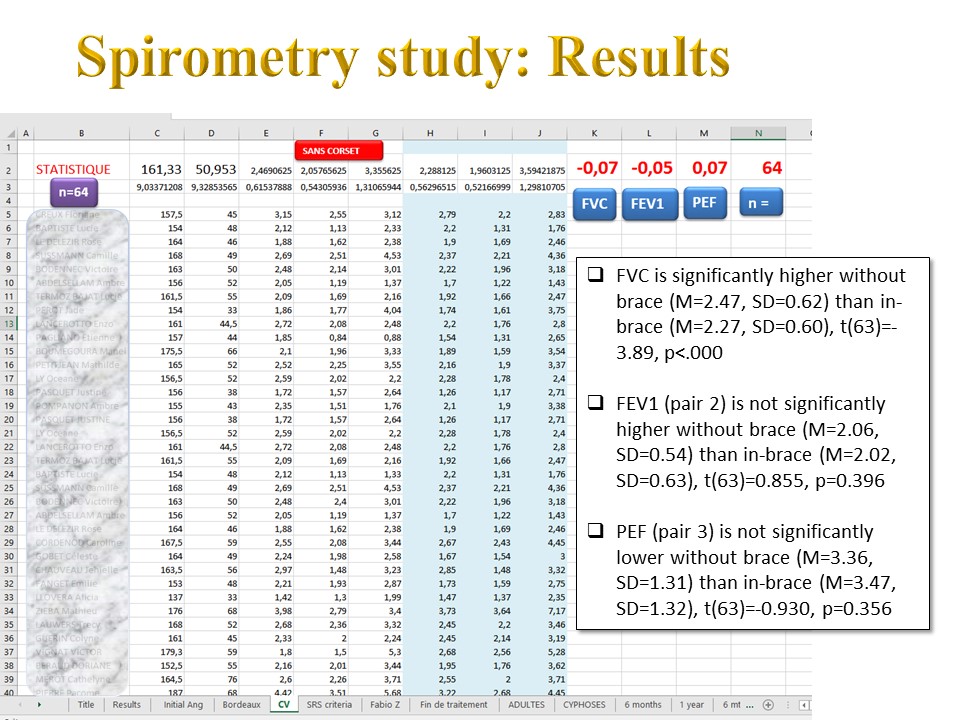 |
Our results were performed on a consecutive series of 64 patients. The in-brace reduction in the vital capacity is only 7% and the peak flow is even improved. |
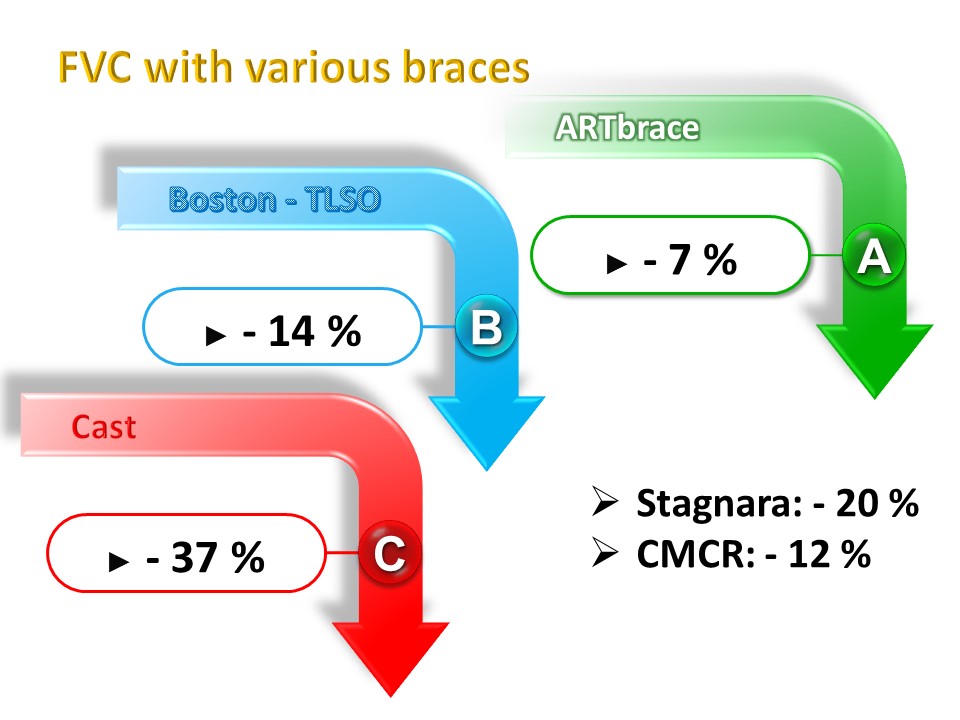 |
Not all braces have the same effect on respiratory function.x |
 |
All braces decrease the FVC, but thanks to its original design, the immediate limitation is only 7%: the lowest reported to date. The other obstructive and mechanical parameters are not significantly modified. |
 |
The brace is the treatment of choice for chest deformities because it is in direct contact with the rib cage. Often associated with a spinal deformity, it is possible to take advantage of the spinal deformity treatment to reshape the thorax. The aesthetic improvement is a compliance factor for the child. In general, the impact of the corset on the vital capacity should be systematically taken into account. |
 |

