 |
|
 |
Scoliosis, the stigma of orthopaedics, is the most difficult vertebral deformity for the doctor to apprehend. The deformity is three-dimensional whereas our imagery is not. The evolution is sometimes linear, sometimes chaotic making therapeutic indications very difficult. The spine is a structure with a tensile integrity which does not support stiffening.
|
 |
|
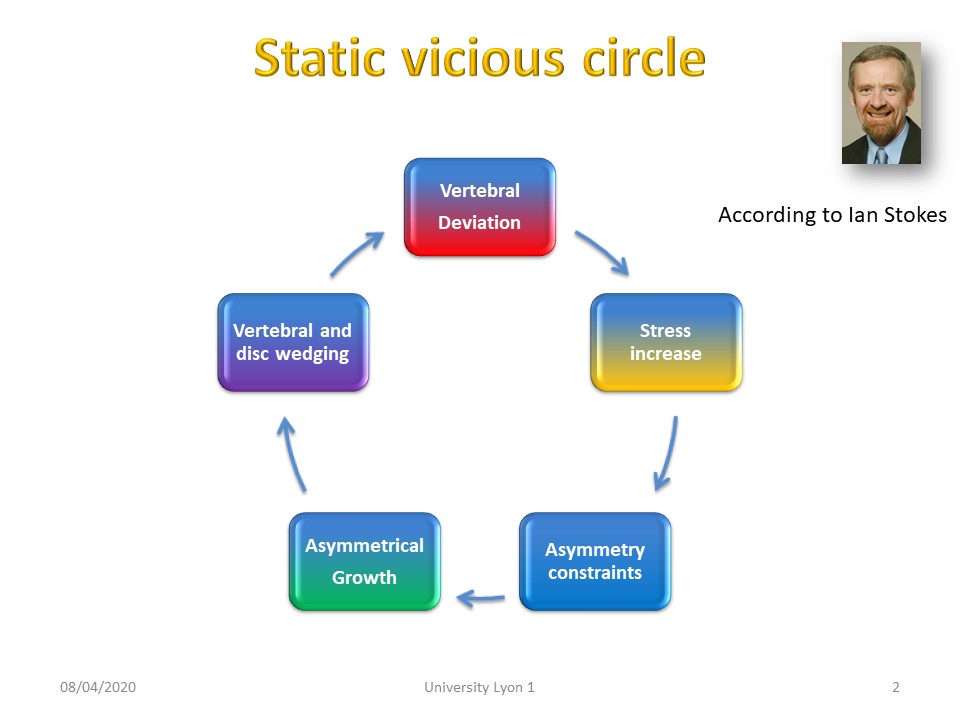 |
During growth, the evolution of scoliosis is linear according to the vicious circle described by Ian Stokes: 1, increased load at apical level 2, This load is even greater in the concavity. 3, Growth is inhibited in the concavity. 4, The apical vertebra is cuneiform, 5, This further accentuates the angulation of the scoliosis.
|
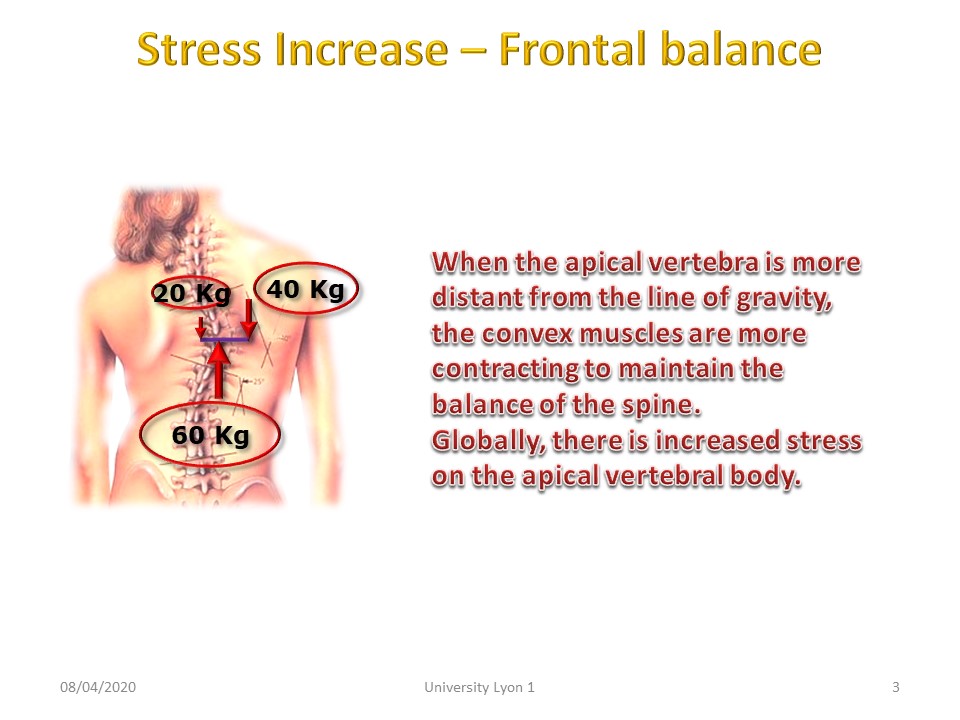 |
As the apical vertebra moves away from the line of gravity, the convex muscles contract further to maintain the balance of the spine (first type of lever arm). Overall, the apical vertebral body is under increased stress.
|
 |
The load increases doubly at the level of the concavity: 1, due to the distance from the line of gravity 2, due to the rebalancing contracture of the convex muscles.
|
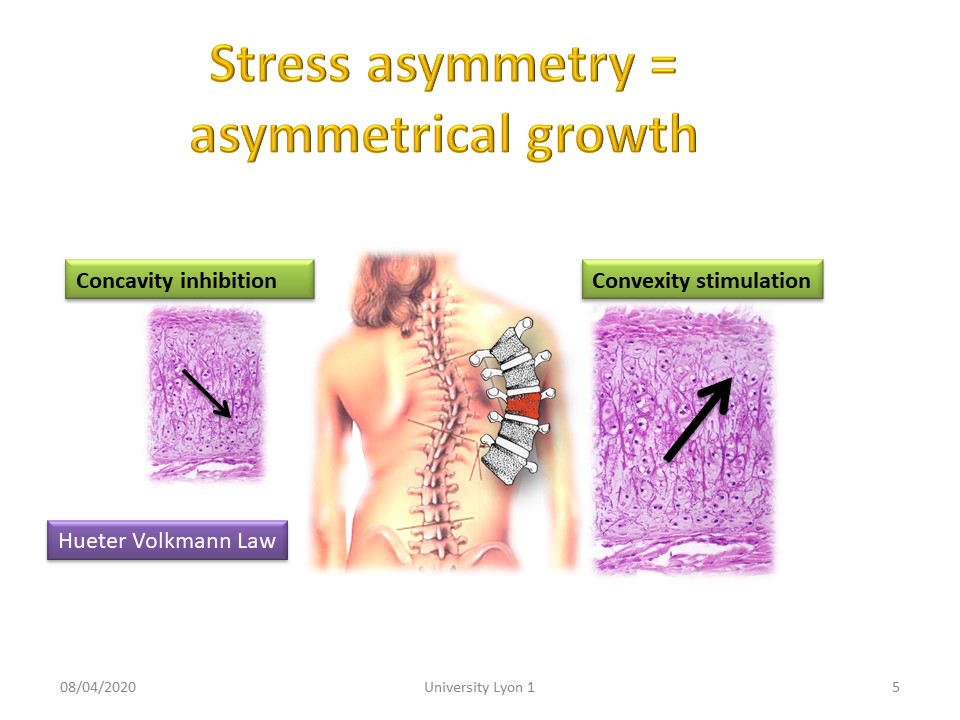 |
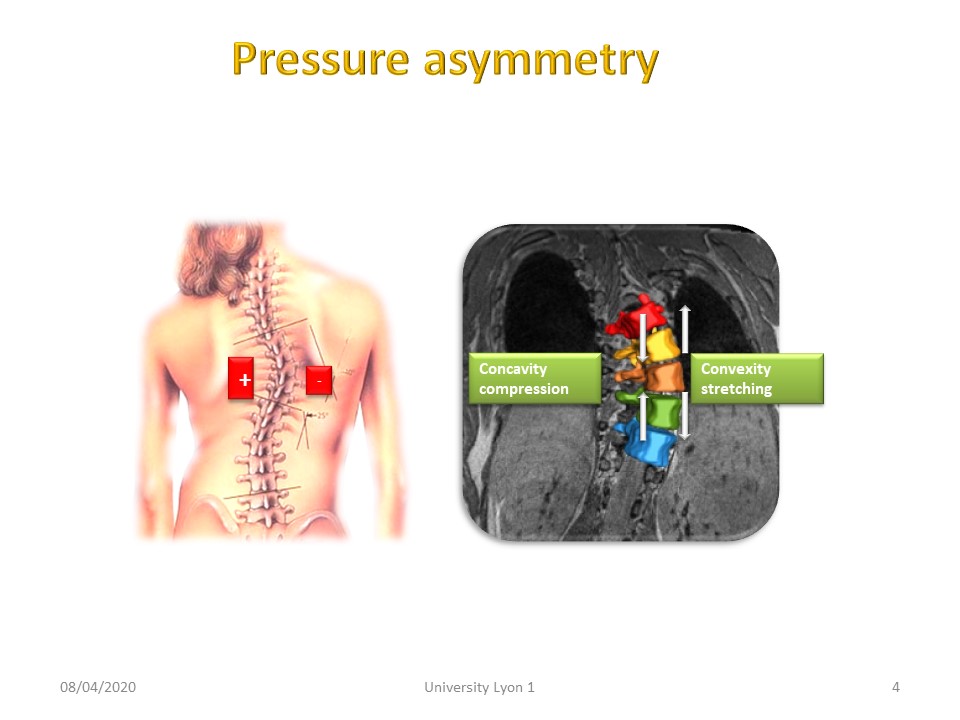
The much greater pressures in the concavity inhibit growth at this level, while convexity is more stimulated.
|
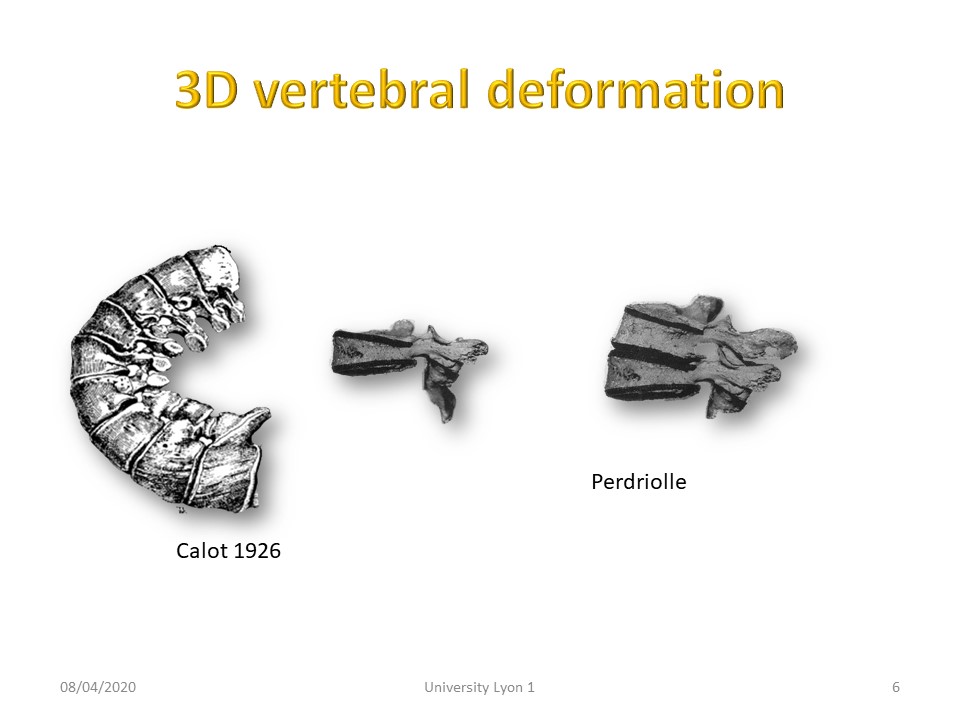 |
This deformation of the apical vertebral body takes place in a 3-dimensional space. When the spine is realigned in a sagittal plane, there is a tendency towards a flat back.
|
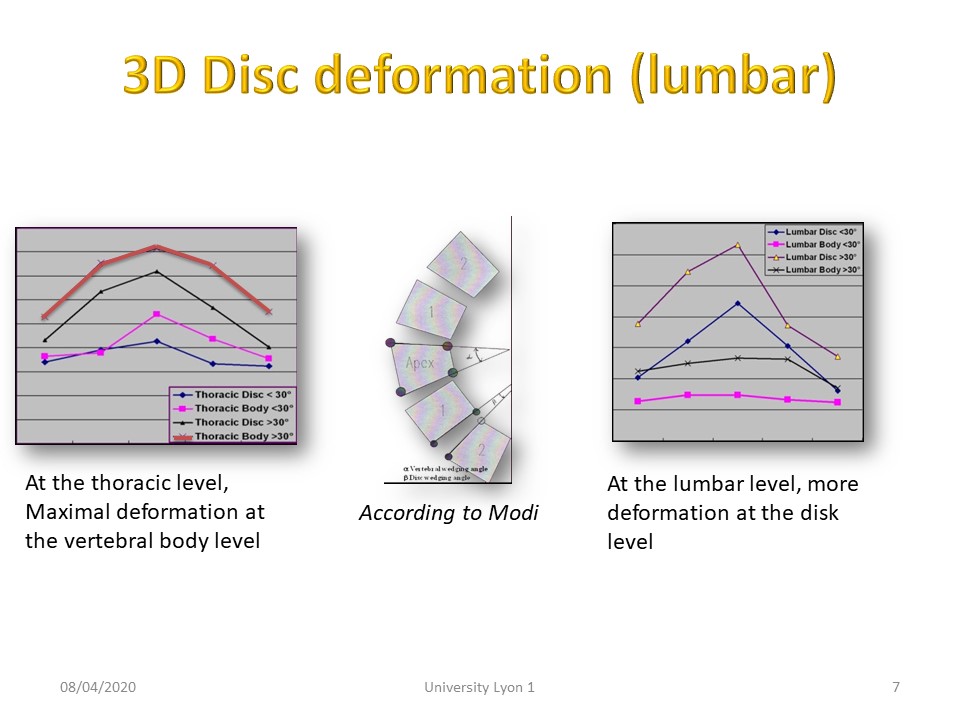 |
Disc deformity predominates in the lumbar region due to the height of the disc, whereas in the thoracic region, bone deformity predominates.
|
 |
|
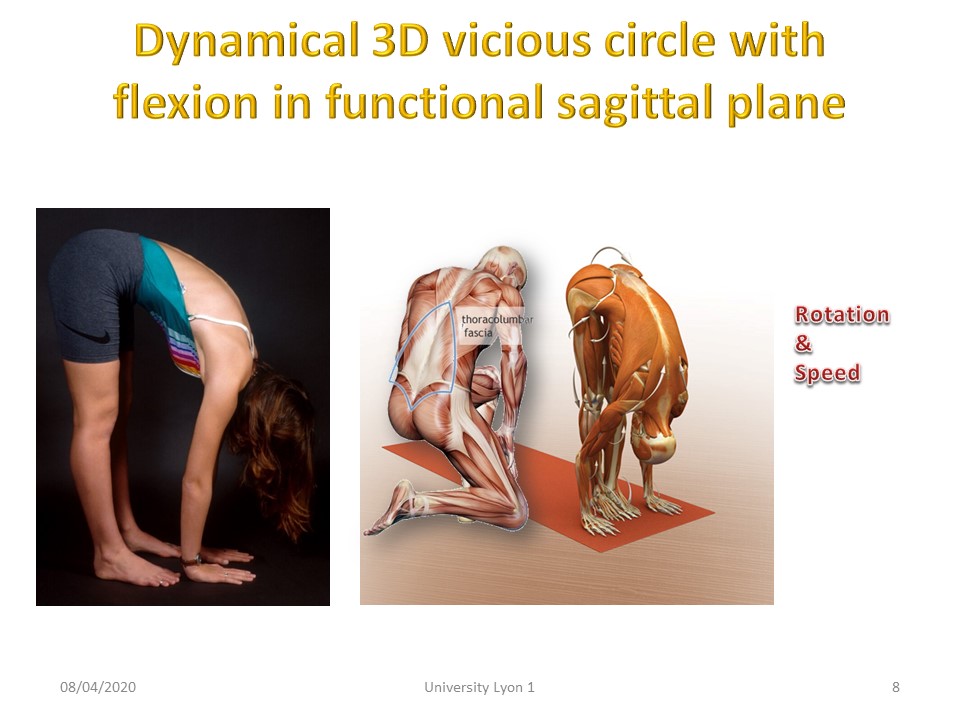 |
These deformations are at the base of a double threshold when the trunk is bent forward.”
|
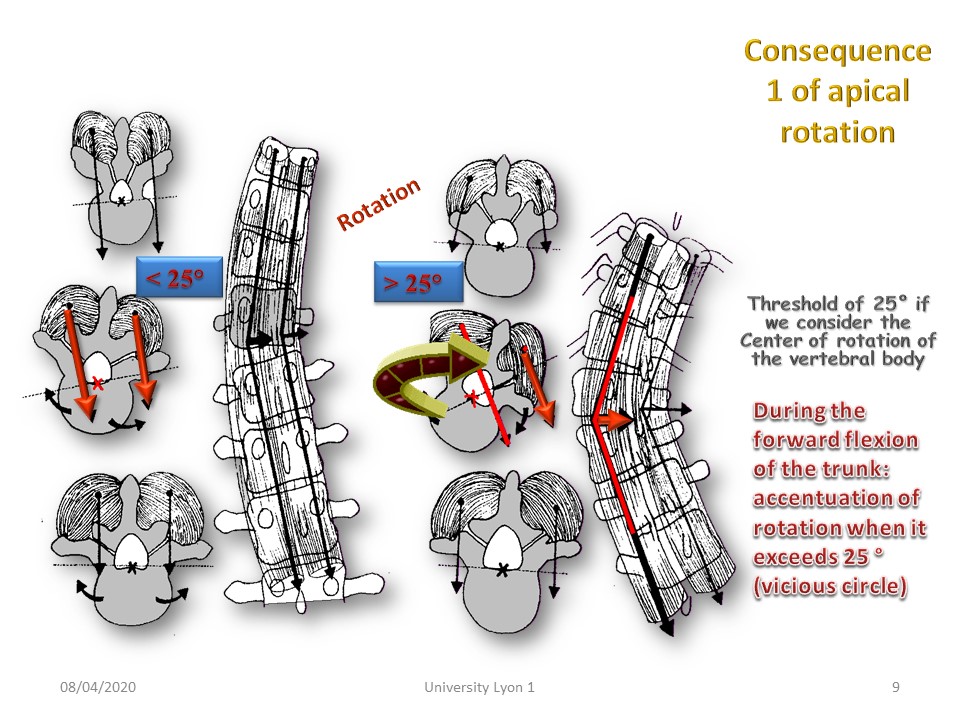 |
When the apical rotation is less than 20°, the vectors of the paravertebral muscles are located on either side of the instantaneous centre of rotation of the apical vertebra and the spine is stable during movement. When the rotation is greater than 25°, the muscle vectors are located towards the concavity but on the same side with respect to the instantaneous centre of rotation, the column is therefore unstable like a bicycle in a too large curve.
|
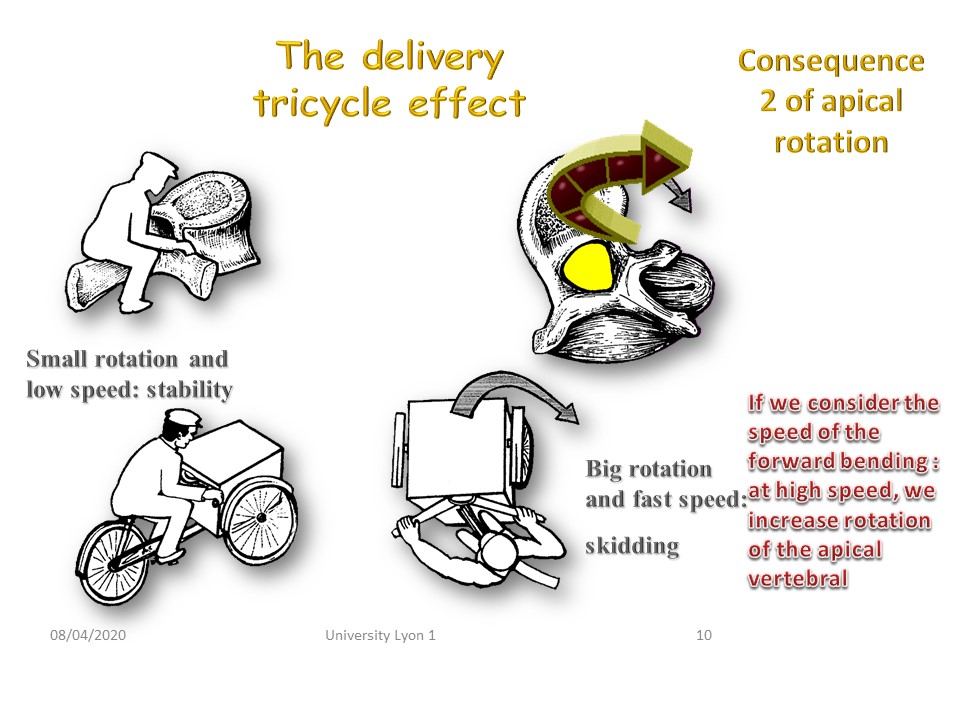 |
The second threshold concerns the speed of anterior bending of the trunk. When bending at a slow speed, there is no problem, but for the same rotation, if the bending is done at a fast speed, the torsional stresses become too high in the disc, which facilitates its degeneration.
|
 |
|
 |
We will now consider the biomechanical consequences in the sagittal plane.
|
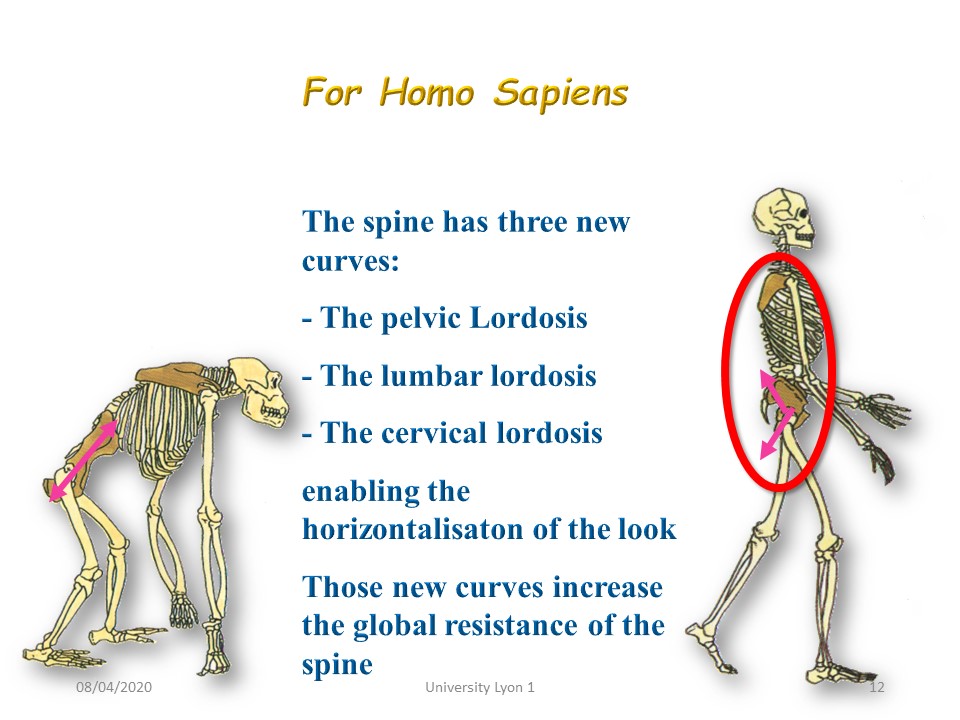 |
In the sagittal plane, the 3 curves allow an almost perfect verticality between the head and the feet on the ground. The gaze is horizontal.
|
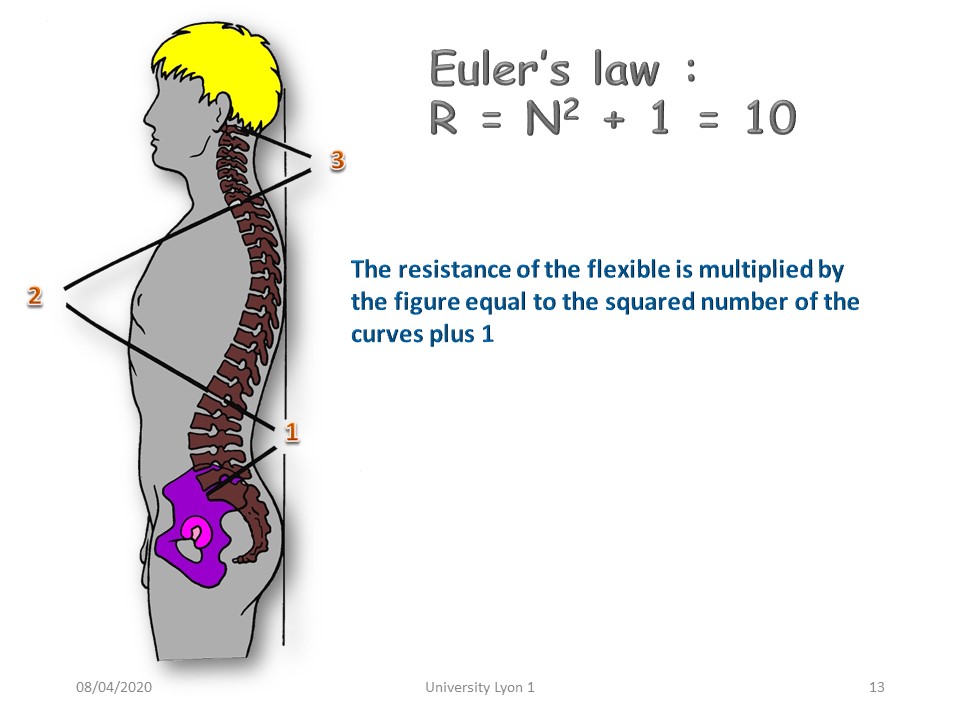 |
Curvatures increase resistance in the sagittal plane. This resistance is theoretically multiplied by 10.
|
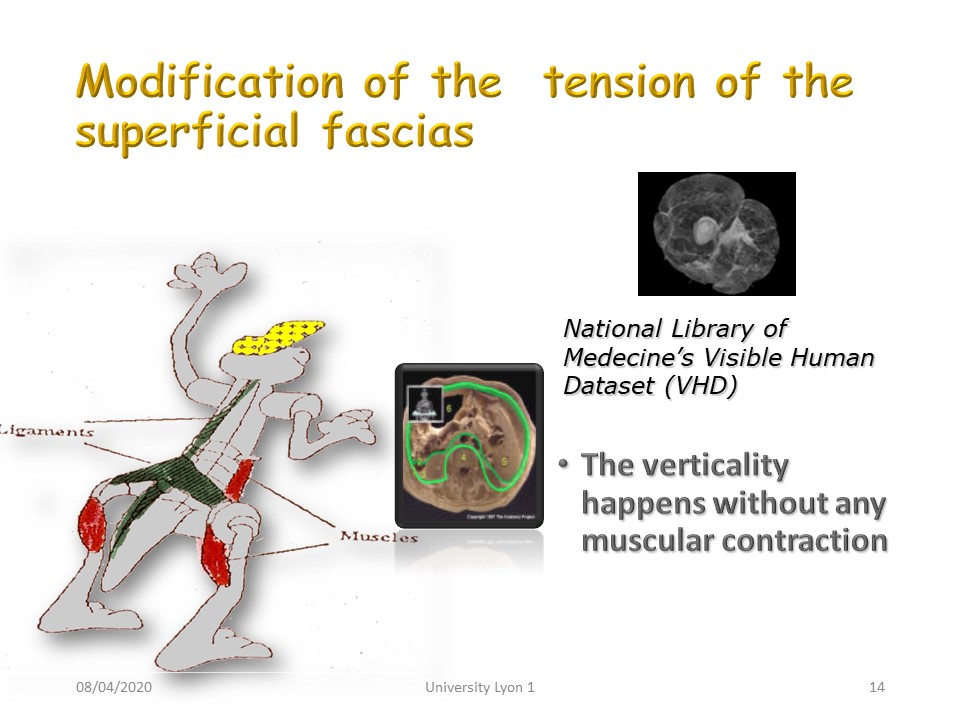 |
With verticality, we observe a transformation of certain muscles into powerful ligaments that allow homo sapiens to remain in an immobile vertical position without voluntary muscle contraction.
|
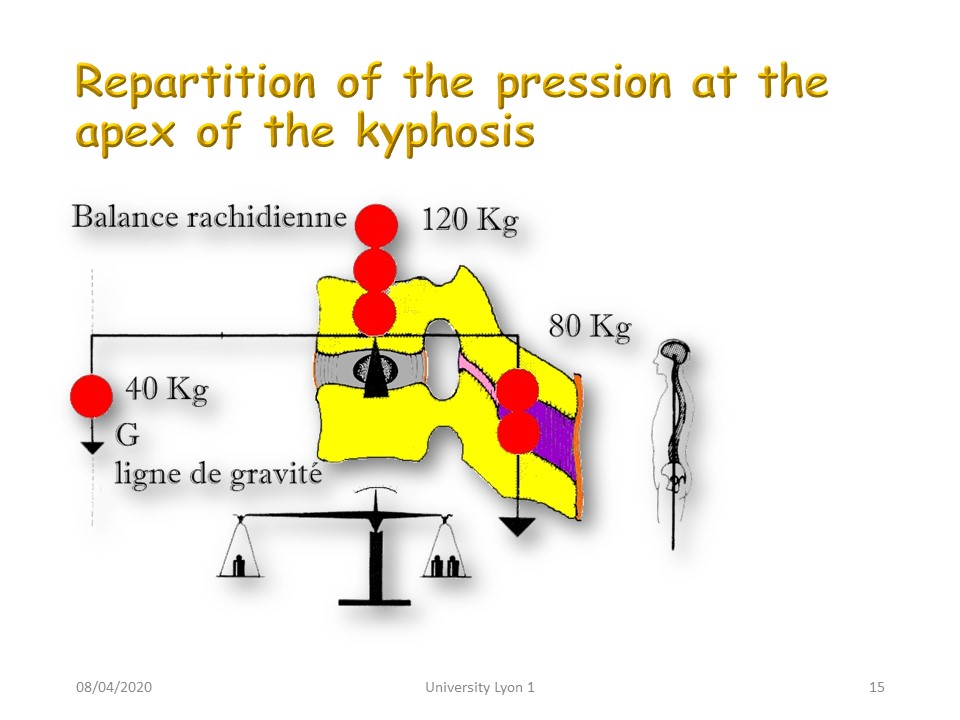 |
As we have seen at the apex of scoliosis, the stresses will be greatest at the apex of sagittal curvatures.
|
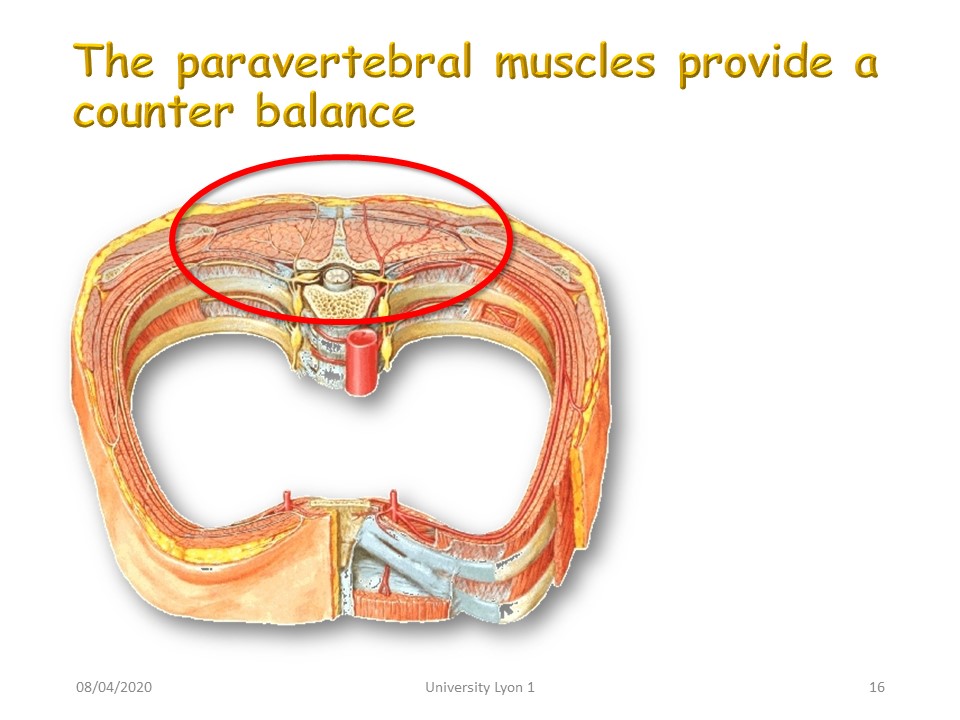 |
At the level of the apex of the kyphosis, it is the posterior musculature which maintains the first class lever arm.
|
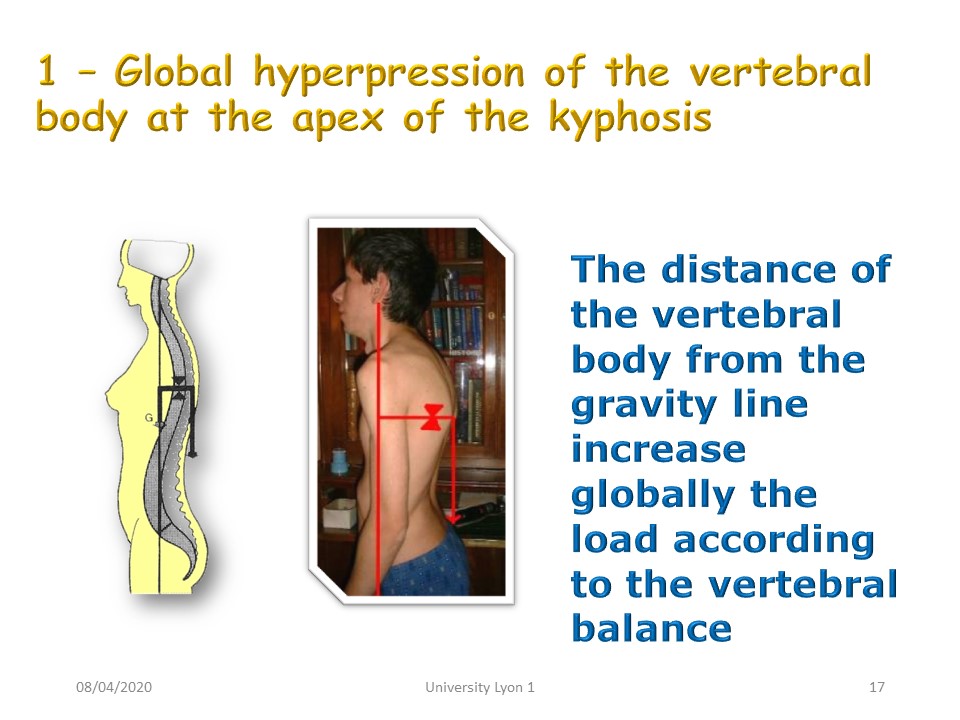 |
What counts is the distance of the apex of kyphosis from the line of gravity without distinction between kyphotic attitude and structural hyper kyphosis.
|
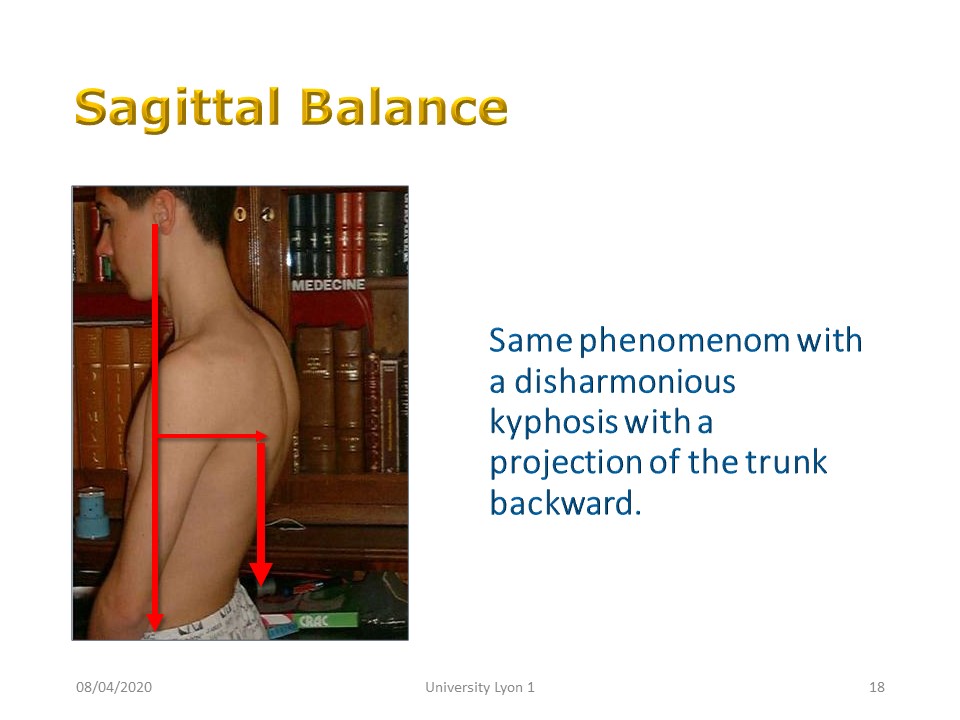 |
The same is true for dysharmonic kyphosis with sometimes pelvic retroversion.
|
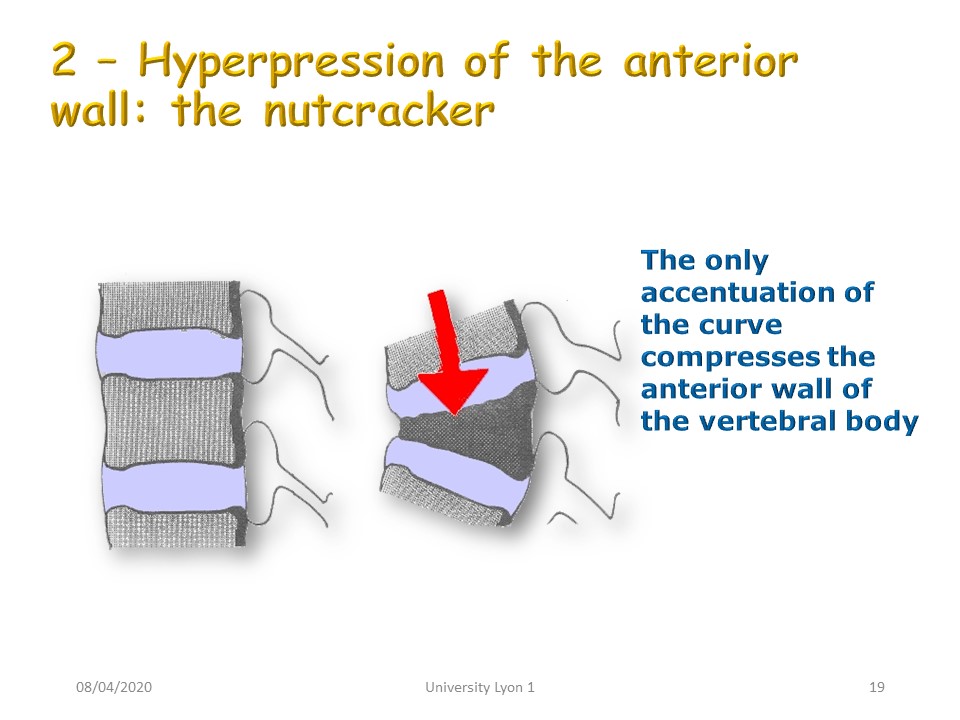 |
The deformation in the sagittal plane causes anterior cuneiformity of the vertebral body which will further accentuate the angulation of the kyphosis. The vicious circle of Ian Stokes also applies to kyphosis.
|
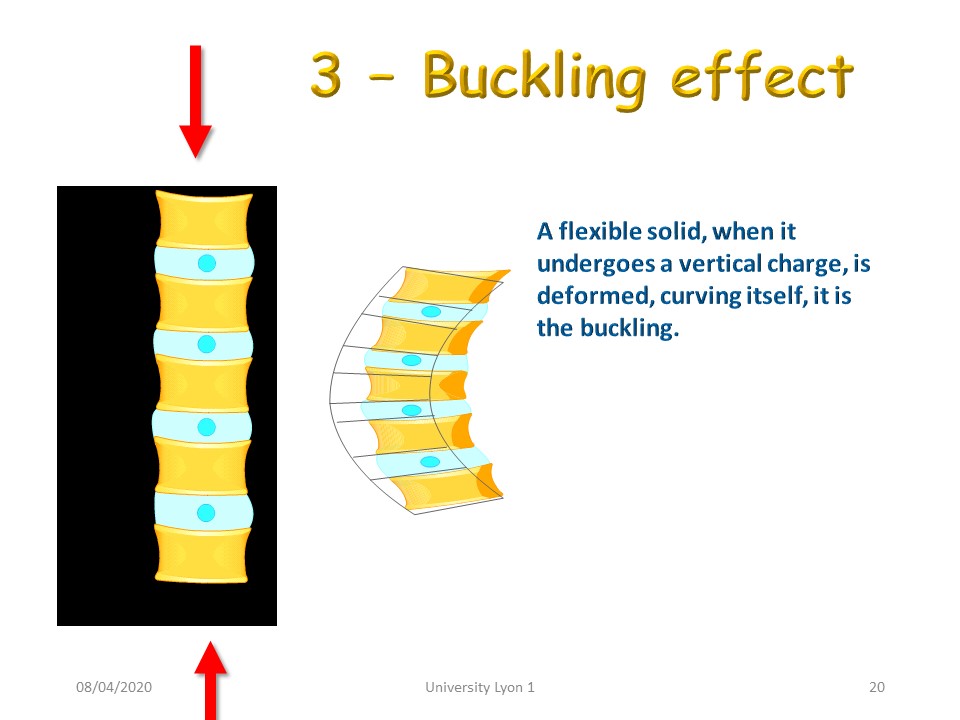 |
Similarly, the buckling effect also applies to the sagittal plane, which probably explains the tendency to accentuate curvatures during adolescence.
|
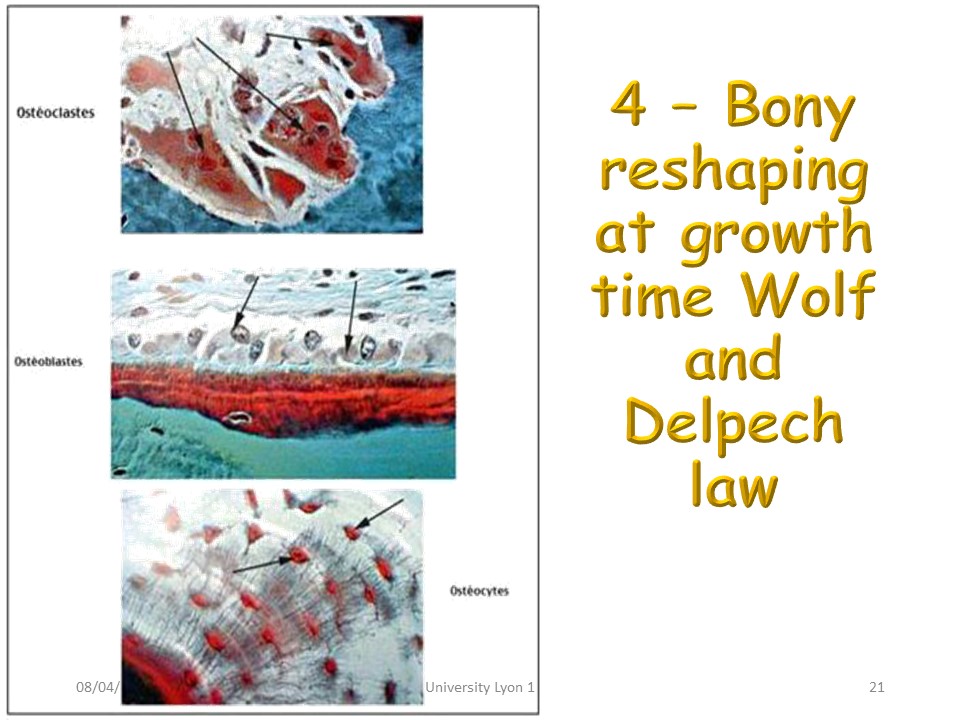 |
Bone remodeling follows Hueter Volkmann's laws with inhibition of bone growth in concavities and stimulation in convexities.
|
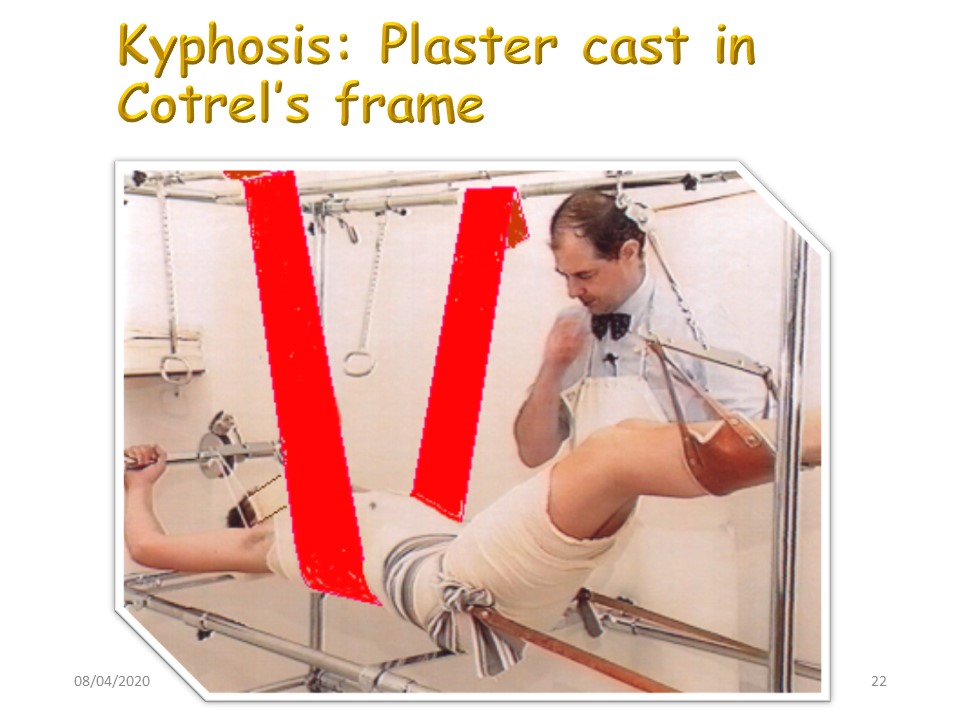 |
As for scoliosis, the Lyon Method of Kyphosis correction involves a reduction in plaster cast preceded by a physiotherapy of stretching. The plaster is retained 1 to 2 months depending on the size and rigidity of kyphosis.
|
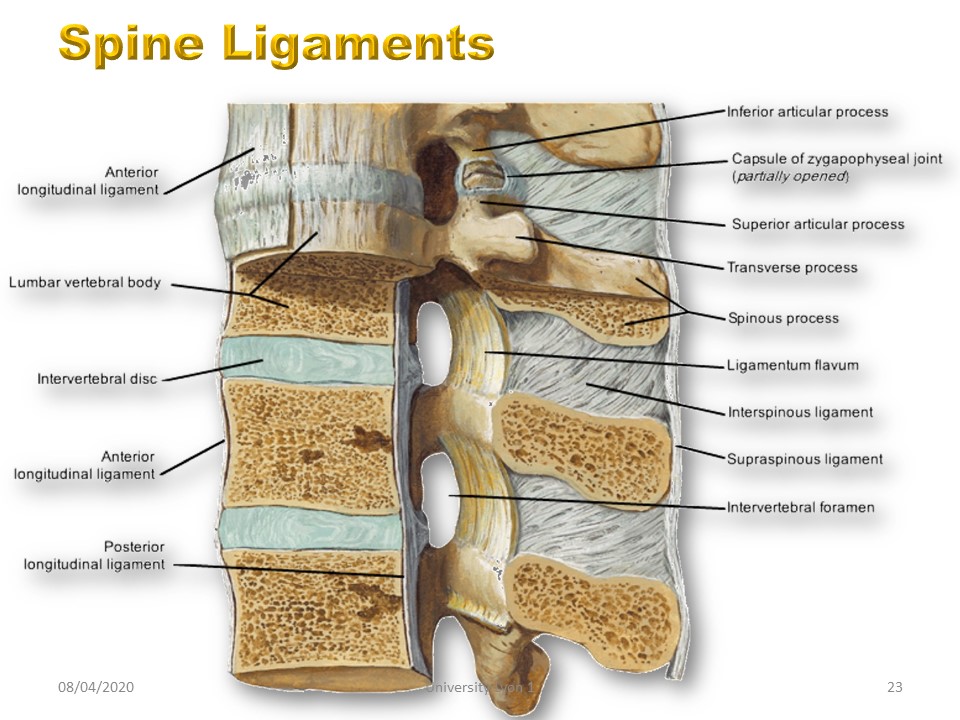 |
Unlike the frontal plane, the ligaments are very strong in the sagittal plane.
|
 |
Unlike the frontal plane, the ligaments are very strong in the sagittal plane.
|
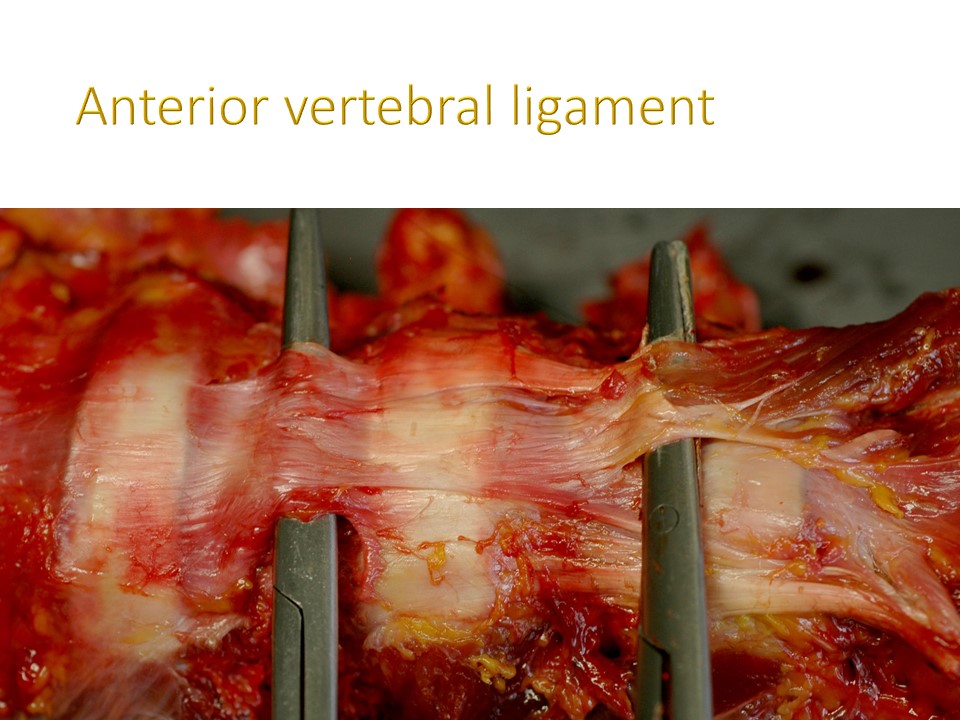 |
The anterior vertebral ligament is very powerful and greatly limits the correction of kyphosis in extension. This is why the plastic deformation at the level of this ligament constitutes the first stage of conservative treatment.
|
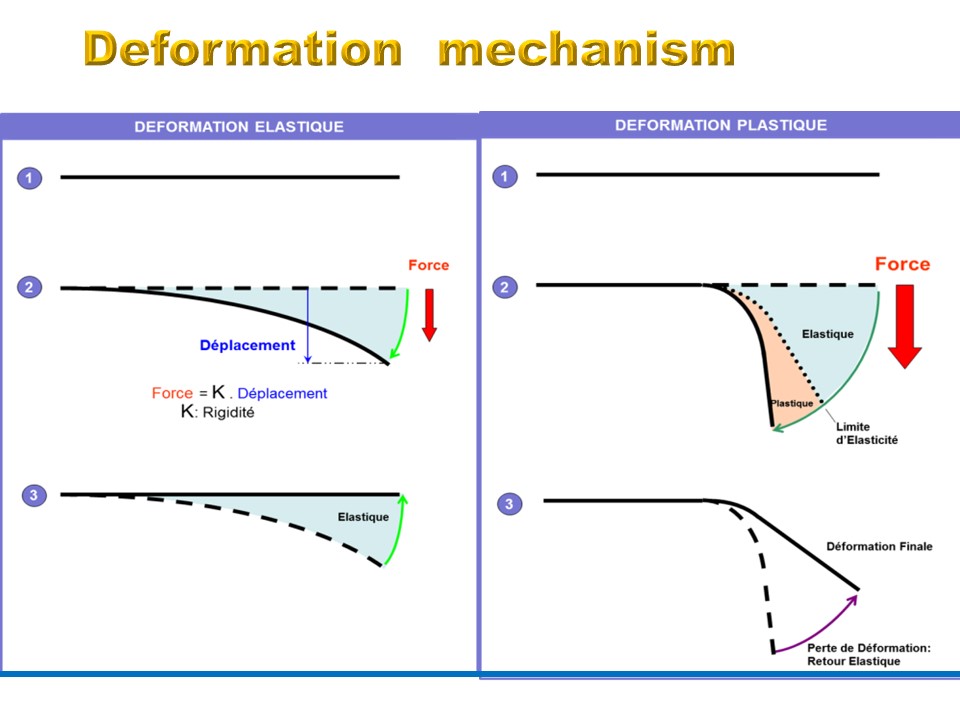 |
A ligament under tension is characterized by: 1. an Elastic behavior (elastic deformation) at the start of elongation, 2. A plastic behavior (plastic deformation) after exceeding the elastic limit,
|
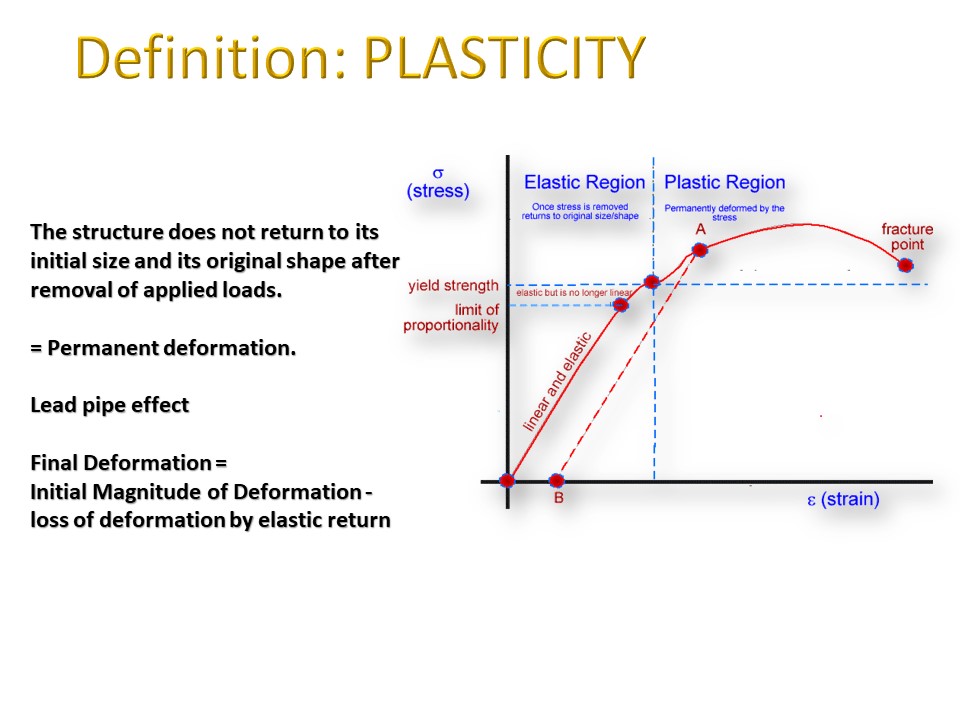 |
In physics and materials science, plasticity describes the deformation of a (solid) material undergoing non-reversible changes of shape in response to applied forces, For example, a solid piece of metal being bent or pounded into a new shape displays plasticity as permanent changes occur within the material itself.
|
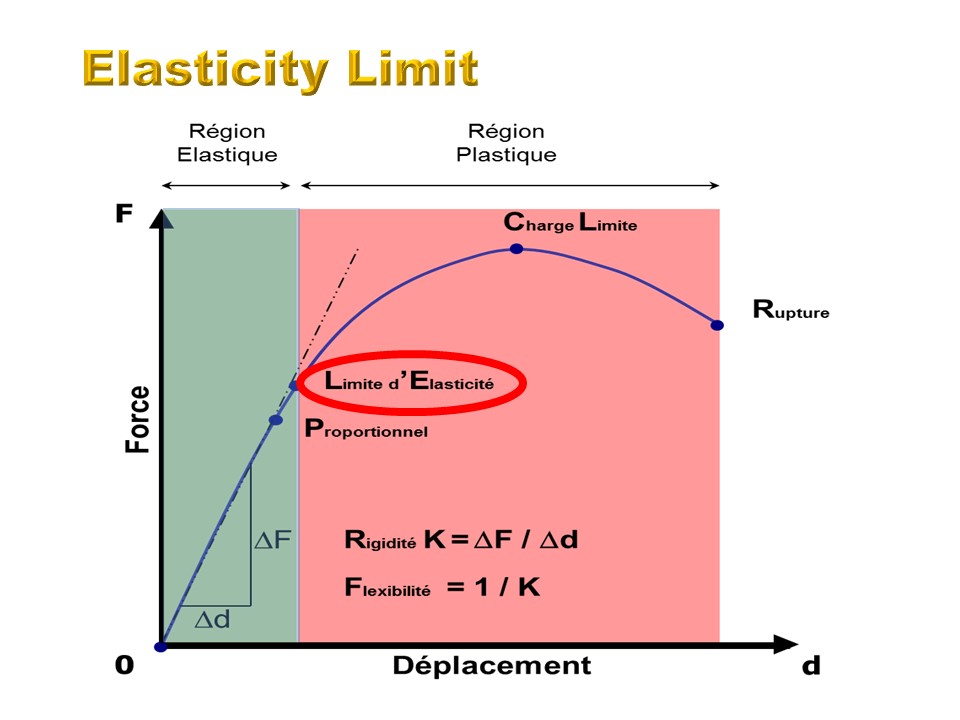 |
The Elasticity limit is exactly the crossing point between: ELASTIC region and PLASTIC region, It’s the maximum stress for the return to the initial state. The elasticity limit is often correlated to the maintenance of the correction: The elasticity limit exceeded, a fraction of the deformation becomes permanent and not reversible, and the correction remains partially.
|
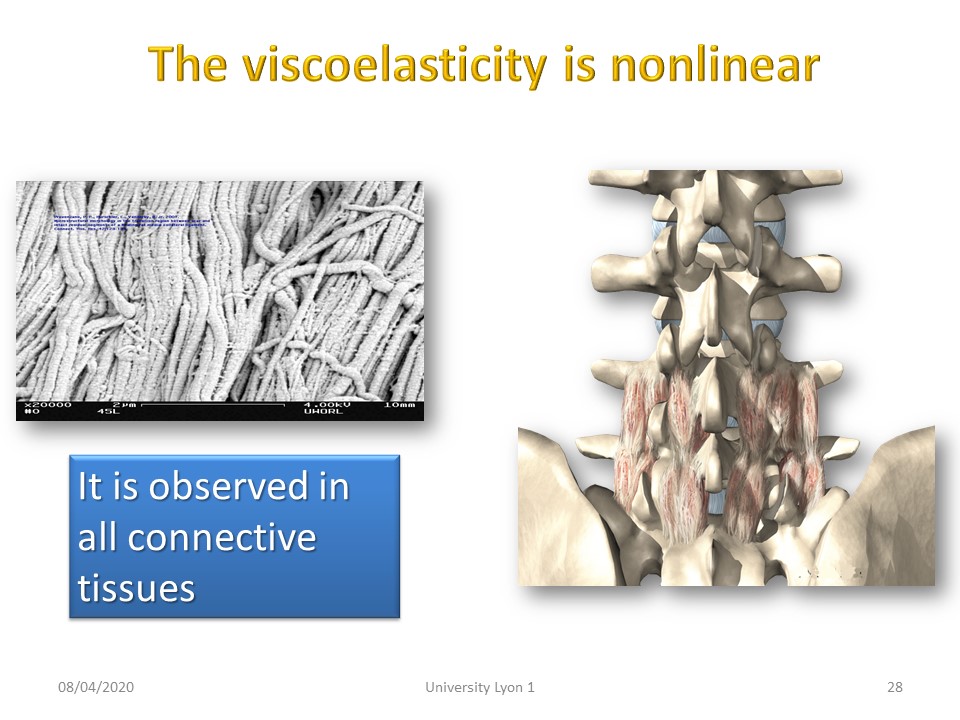 |
Tensegrity is a non-linear system, like the viscoelasticity of our paravertebral connective tissues.
|
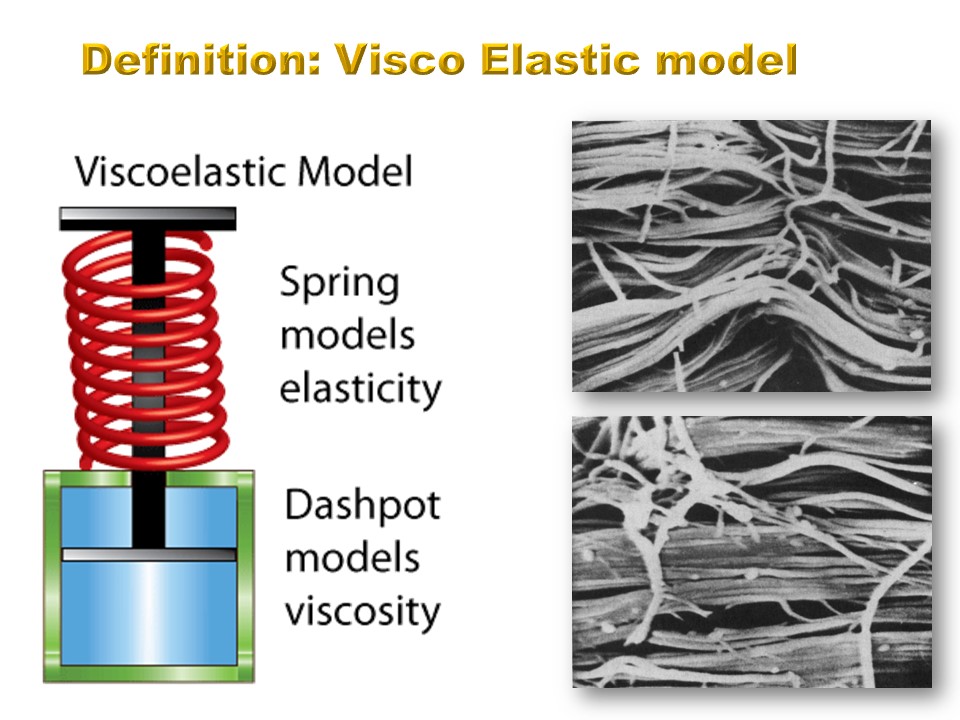 |
When an elastic material containing fluid is deformed the return of the material to its original shape is delayed in time and it is slower to restore to its original position.
|
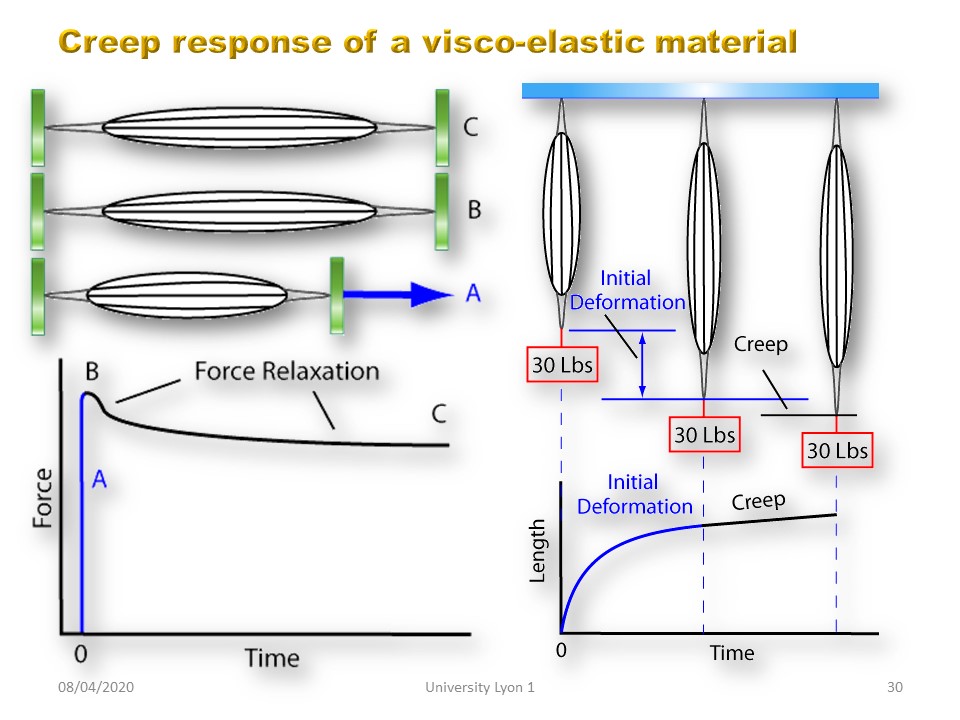 |
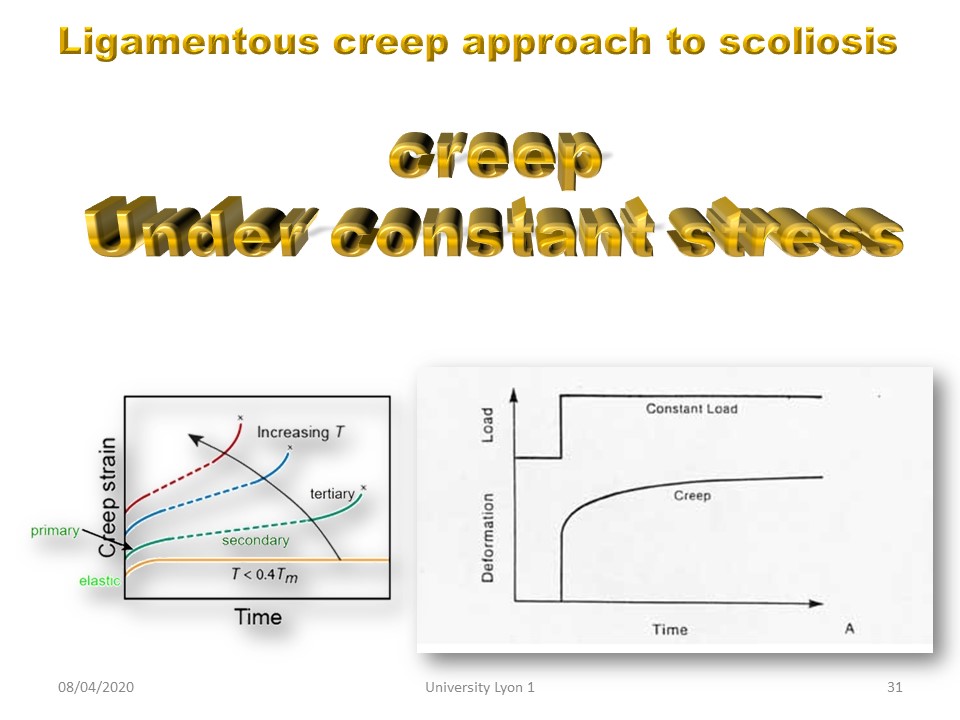
In materials science, creep (sometimes called cold flow) is the tendency of a solid material to move slowly or deform permanently under the influence of mechanical stresses. It can occur as a result of long-term exposure to high levels of stress that are still below the yield strength of the material.
|
 |
The tissue response to load is dependent on: 1. Magnitude of load (ie quantity of hypercorrection) 2. Duration of load (from 1 to 4 months) 3. Prior loading (hysteresis). The magnitude of load is limited by the tolerance of the child and only sporting activity can cause hysteresis; phenomena usually leading to fragilizations and ruptures of the tendon. The only parameter available to us is the duration of the cast or total time correction. So Creep is the time dependent elongation of a tissue when subjected to a constant stress. For kyphosis 4 to 8 weeks are needed to achieve sustainable elongation.
|
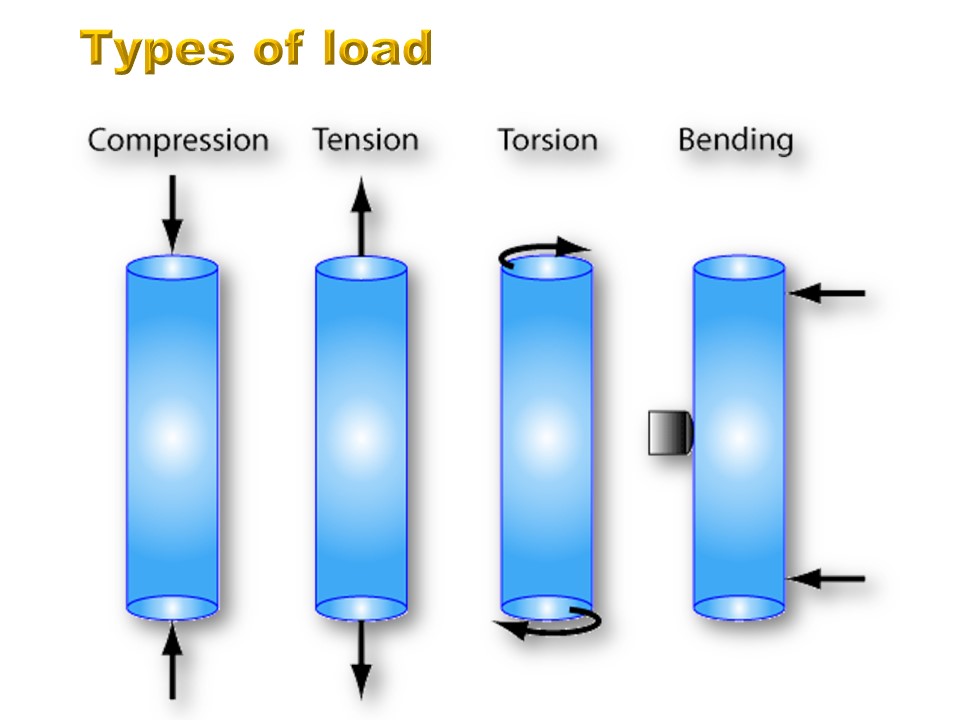 |
These laws are valid regardless of the type of load. Stagnara's Lyon brace works mainly in compression and bending. The new Lyon ARTbrace Lyon works in torsion. For kyphosis we use mainly posterior compression and anterior tension.
|
 |
These laws are valid regardless of the type of load. Stagnara's Lyon brace works mainly in compression and bending. The new Lyon ARTbrace Lyon works in torsion. For kyphosis we use mainly posterior compression and anterior tension.
|
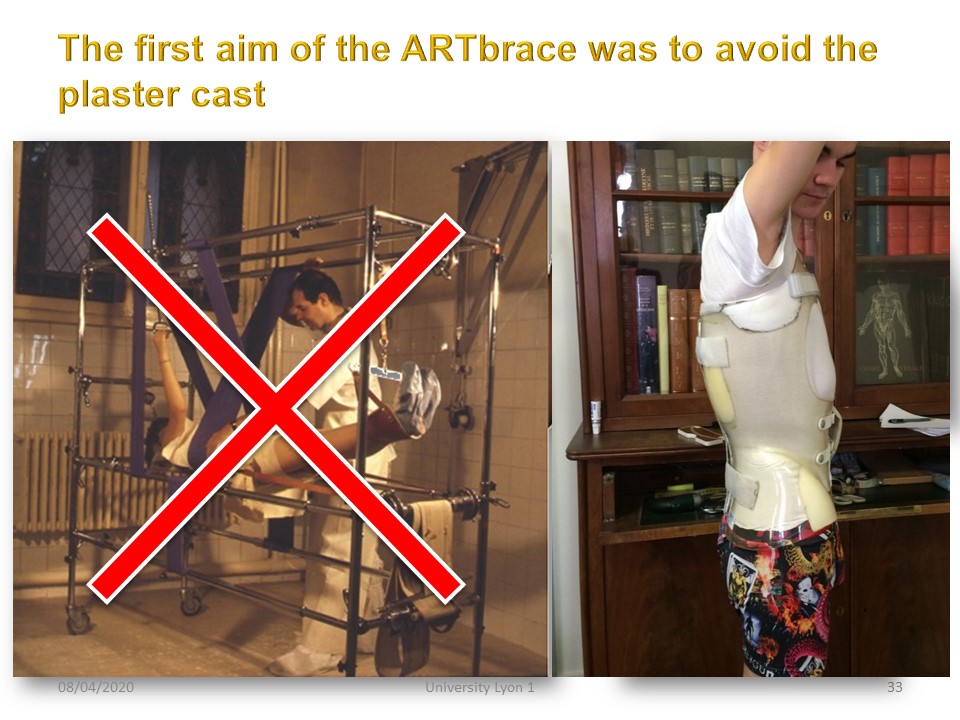 |
The current technology of regional shape capture allows us to realize an immediately corrector brace. The “total time” in polycarbonate will then be the equivalent of the cast.
|
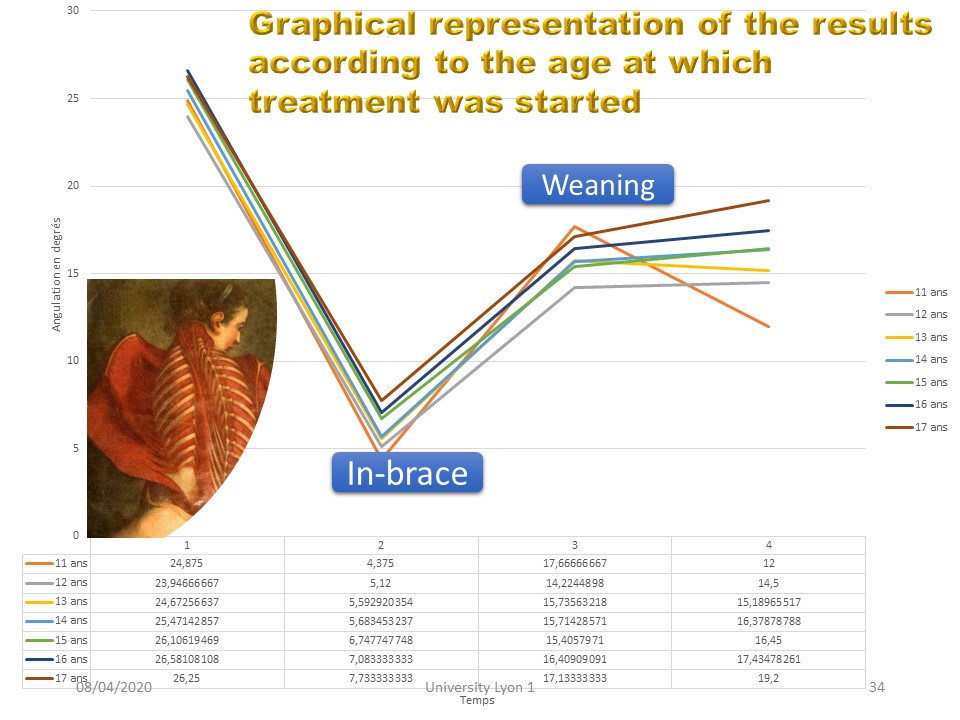 |
In recent work on the results of short lumbar braces, it was found that this creep effect on the viscoelastic paravertebral structures does not depend on the age of the patients. The angular correction curve is identical whatever the initial age at which treatment is started.
|
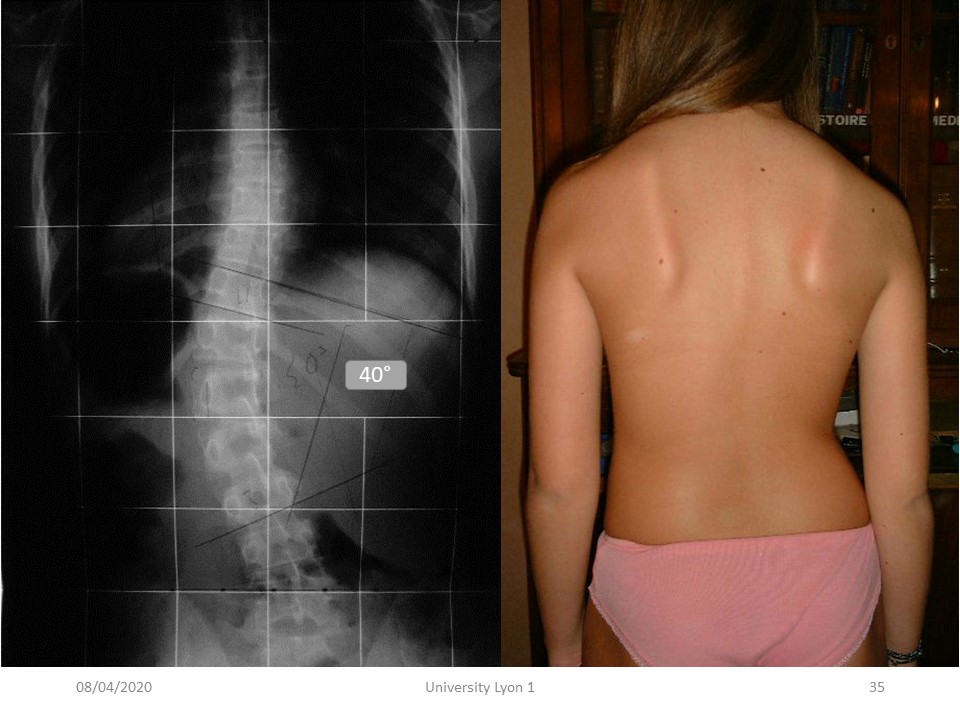 |
Here is an example of lumbar scoliosis with excluded pelvis and an initial angulation of 40°.
|
 |
The rotation was very significant.
|
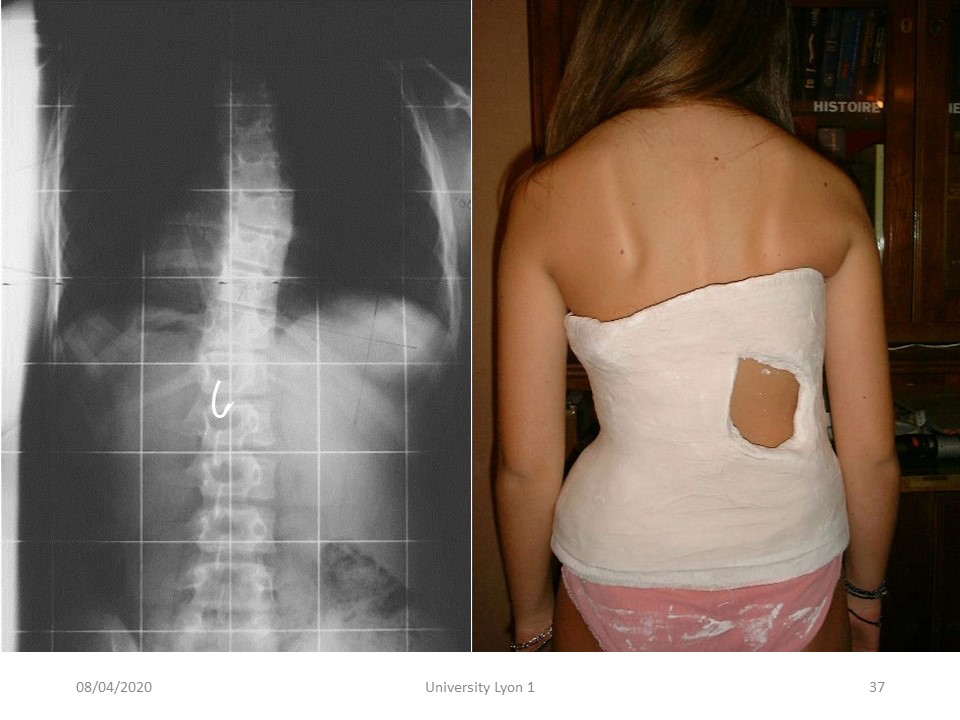 |
The correction is excellent in the frontal plane, but also horizontal since the rotation of T12 passes in the opposite direction. I made this cast myself 30 years ago in lordosis and frontal shift without any direct action in the horizontal plane.
|
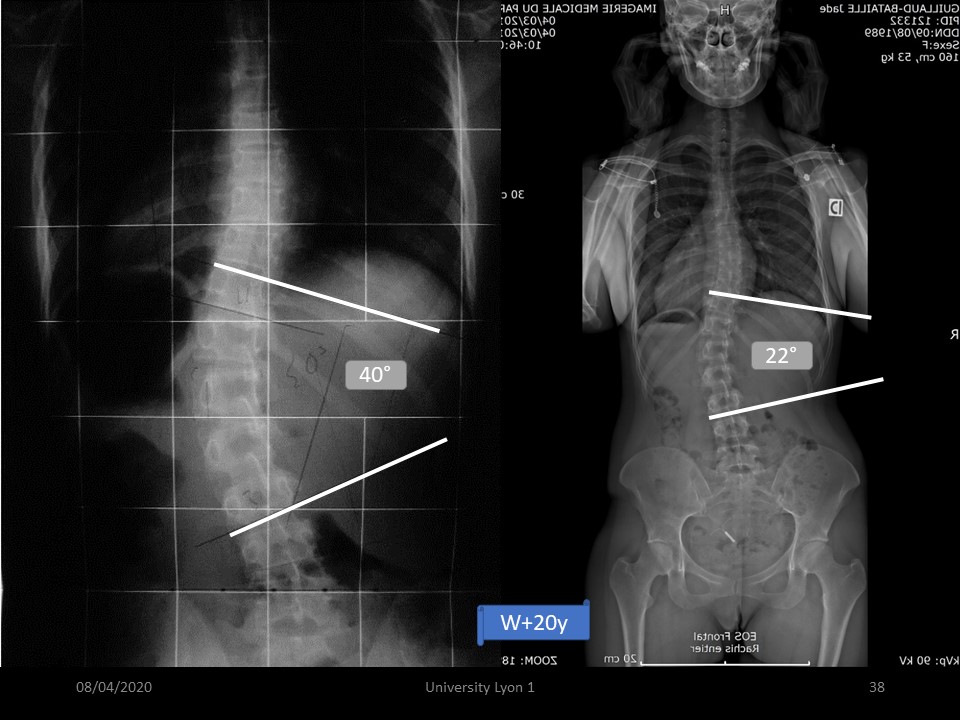 |
The final result 20 years after brace weaning is very correct.
|
 |
Another advantage of the initial “total time” is that the permanent contact of the brace on the skin decreases the sensitivity of load. (Manuel Rigo)
|
 |
|
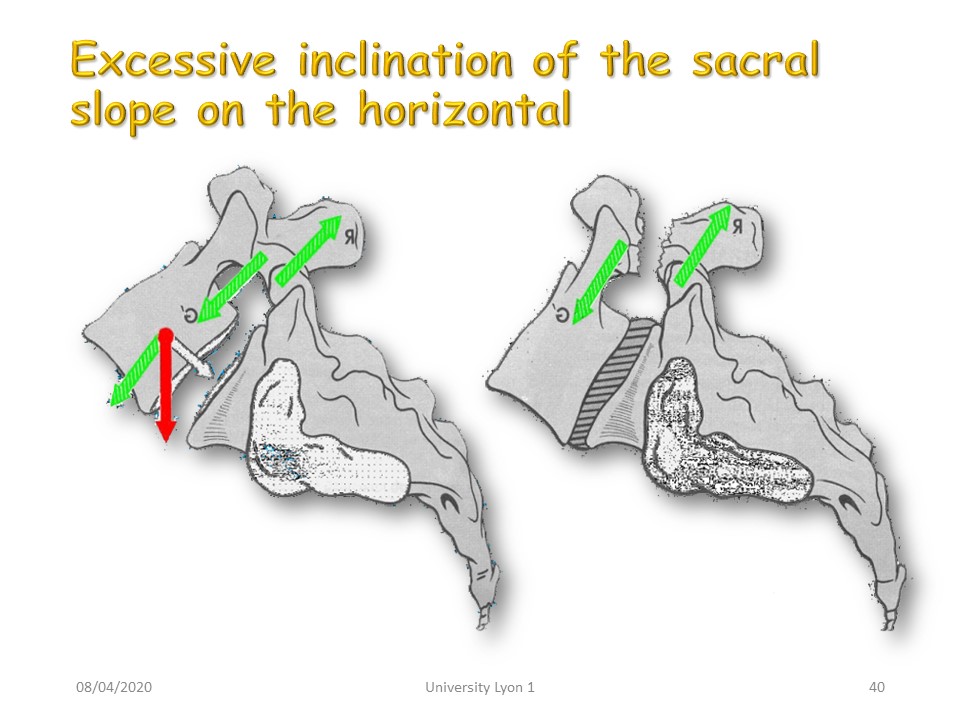 |
The biomechanics of the lumbo-sacral hinge is based on the decomposition of the parallelogram of forces. The force applied to the centre G of the vertebral body is decomposed into a white arrow perpendicular to the plateau of S1 and a green arrow of sliding with shear effect at the pars interarticularis of the posterior arch. The more the sacral plateau is inclined, the greater this component will be.
|
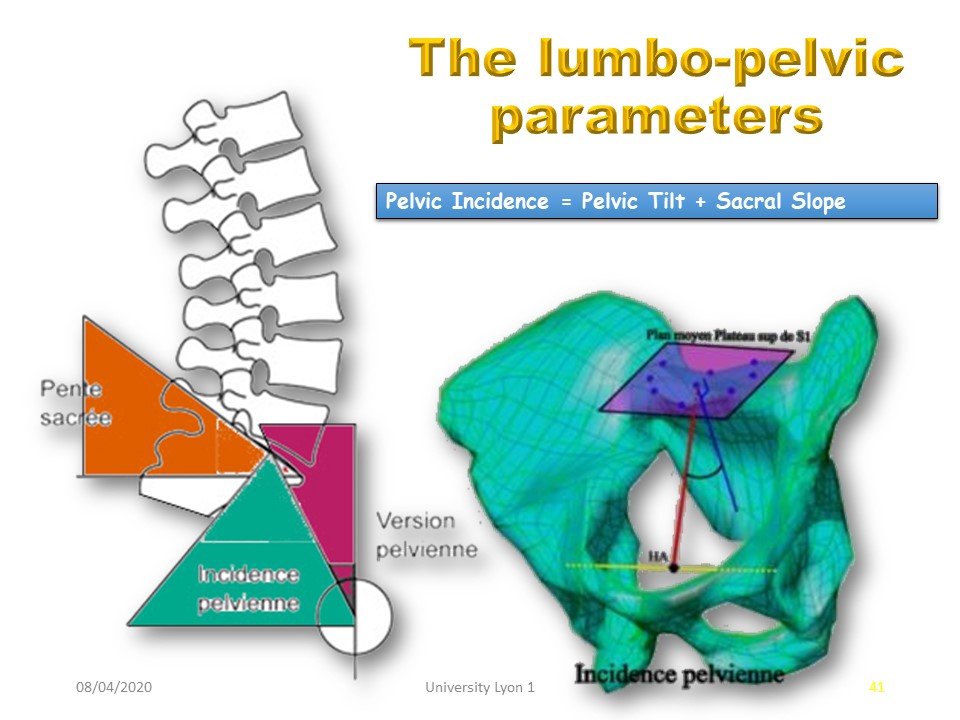 |
The inclination of the sacred slope is linked to the lumbo-pelvic parameters defined by Mrs Duval-Beaupère. Pelvic incidence is a constitutional parameter between the femoral head and the sacrum. It is equal to the sum of the pelvic version and the sacral slope. The sacral slope is correlated with lordosis. The adjustment is made by the pelvic version.
|
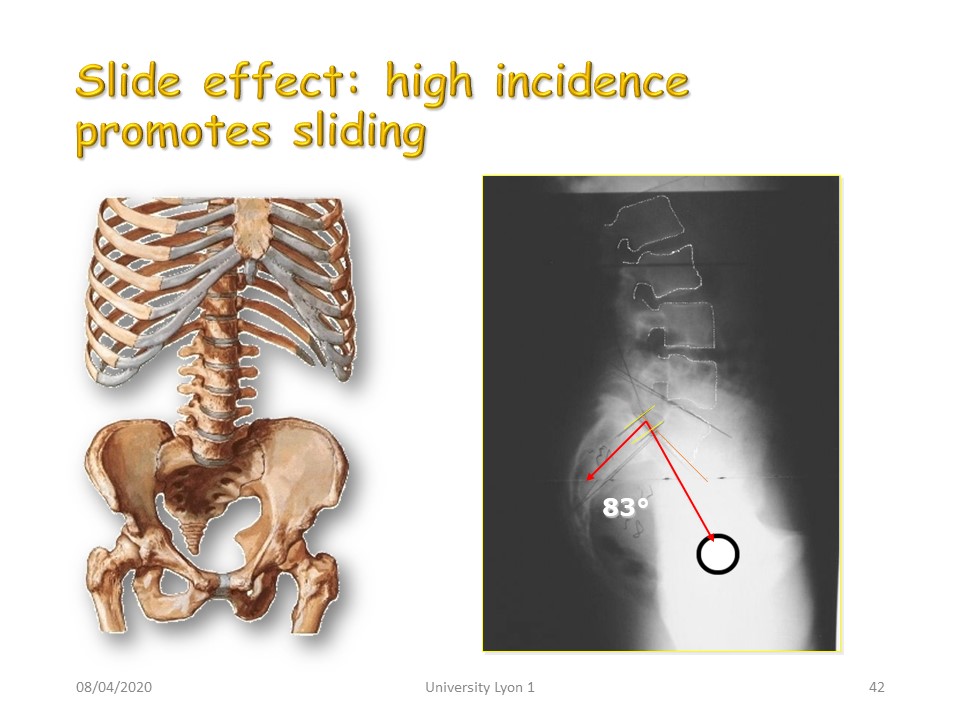 |
Hyperlordosis with a high lumbo-pelvic incidence will favour spondylolisthesis. They will often require the use of a brace.
|
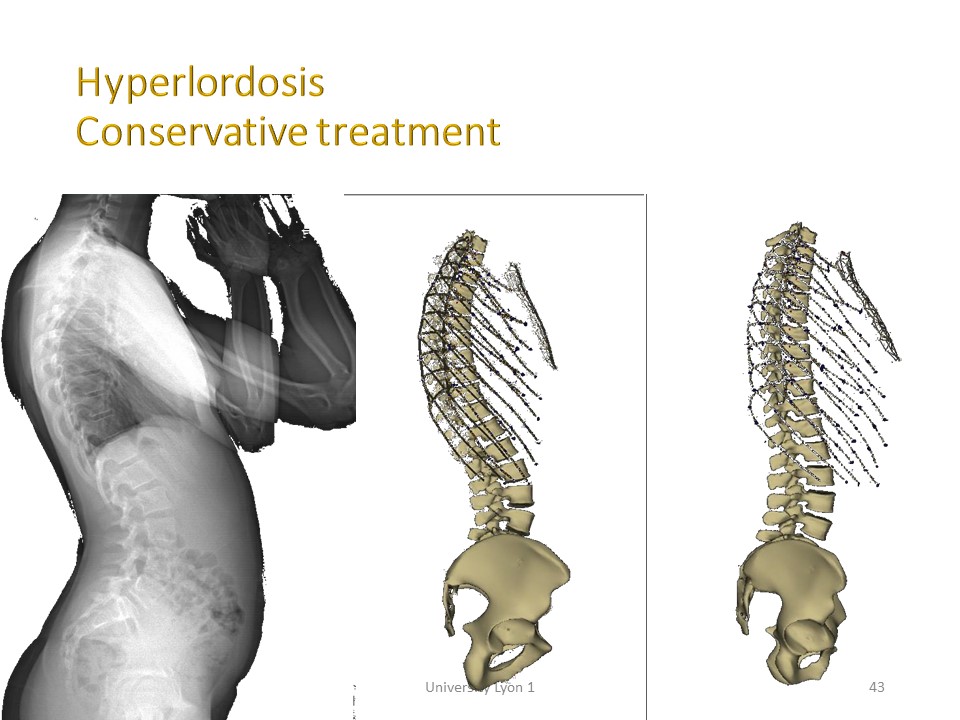 |
Hyperlordosis with physiological lumbo-pelvic incidence will be treated by postural correction with pelvic retroversion by toning the abdominal and gluteal muscles.
|
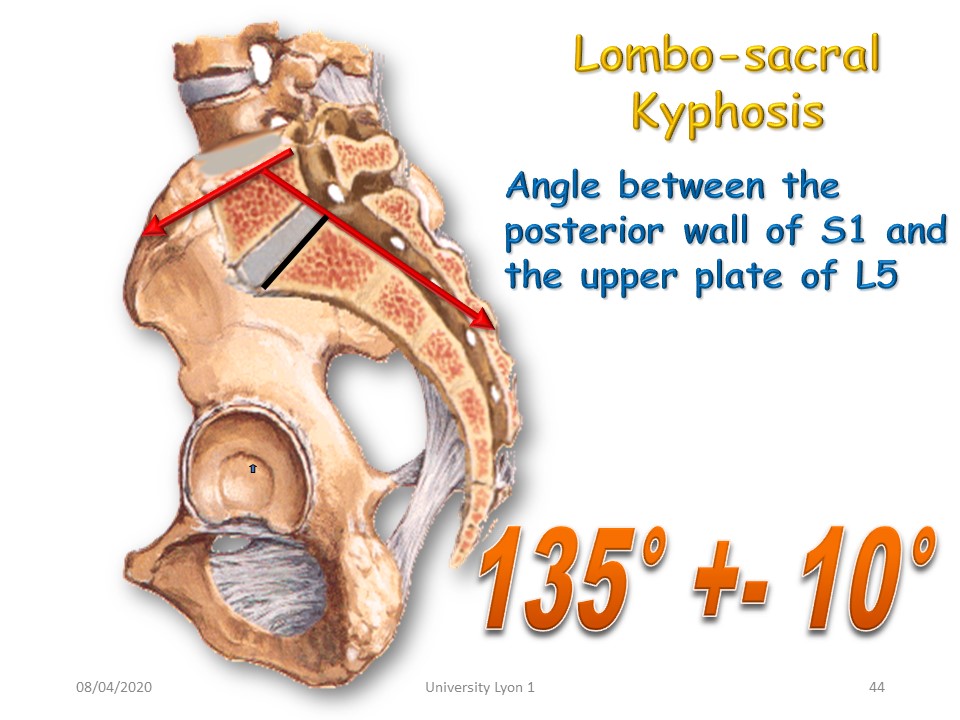 |
Another constitutional factor involved in spondylolisthesis is lumbo-sacral kyphosis, which takes into account the shape of the sacrum and the possible cuneiformization of L5. This angle can be assimilated to the slope of a roof, the lower the angle, the steeper the roof and the greater the sliding component.
|
 |
Another constitutional factor involved in spondylolisthesis is lumbo-sacral kyphosis, which takes into account the shape of the sacrum and the possible cuneiformization of L5. This angle can be assimilated to the slope of a roof, the lower the angle, the steeper the roof and the greater the sliding component.
|
 |

To register for Certification, please contact SSOL

|
")
")
")
")
")